Elizabeth Jones, MT, ABHI (CHT), ASPT (CPT)
- Instructor
- Medical Laboratory Program
- Community Technical and Adult Education Center
- Allied Health Department
- Ocala, Florida
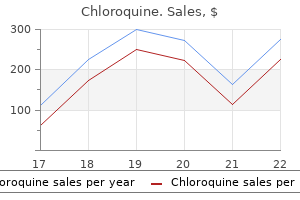
Four of the respondents were radiologists who used both the core and vacuum biopsies with tomosynthesis during the evaluation treatment toenail fungus purchase chloroquine with paypal. Another commented that the angle of approach allowed good visualisation of pre-fire position and the greater space between the tube head and the biopsy device meant that the gun could be rotated through 90° when taking samples medicine mound texas 250mg chloroquine amex. One comment was that the touchscreen had nice graphics showing the needle and lesion position medicine dictionary chloroquine 250mg generic. There was one comment about multi-sampling needing several separate manipulations of the controls atlas genius - symptoms buy on line chloroquine. One comment was that the software was easier to use with the automatic repositioning facility art of medicine buy cheap chloroquine 250 mg on-line. One commented that it was good for masses and distortions administering medications 7th edition ebook buy generic chloroquine 250 mg online, but very poor and not reliable for calcium. The other comment was that it was good to have a facility to view the whole breast as well as the initial targeted area. The respondent who said average liked the Multi-Pass facility included in the upgrade. Of those who found it excellent, one radiologist said that tomosynthesis biopsy was quicker and easier, especially with distortion which may only be seen in one of the pair of images in conventional 2D imaging. She also 24 Practical evaluation of Hologic Affirm breast tomosynthesis biopsy system said that it was easier to target with tomosynthesis. One advanced practitioner who had responded excellent also said that tomosynthesis was excellent for distortion and good for calcium, but poor for fine calcium. Only one of the advanced practitioners responded to the questions as she had had more opportunities of following the relevant training. Out of the seven respondents, there were a total of five who responded to the questions on vacuum biopsy. The last one gave no rating, but commented that it was difficult with diffuse calcium, but very good with distortions. There was good patient feedback with two ladies who had had initial 2D conventional core biopsies finding the vacuum biopsies less painful or uncomfortable, although both had more bruises. Access to these systems is restricted to authorised users only, by password protection. Training All the radiologists and advanced practitioners were trained and experienced in the use of tomosynthesis for assessments as described in an earlier practical evaluation. In addition, they each received individual training at the centre in the use of the Affirm system and vacuum biopsy, and in tomosynthesis biopsy, from the Hologic applications specialists. The majority of radiographers were already trained and experienced in operating the Selenia Dimensions in tomosynthesis mode. All those involved in this practical evaluation received further training from the Hologic applications specialist before operating the Affirm tomosynthesis biopsy equipment at the centre. The Hologic applications staff provided the training on site both at the beginning of the evaluation, and also after the software upgrade which took place about half way through the evaluation. The decubitus position is the position of choice by the unit’s practitioners for the majority of biopsies, as it minimises vasovagal episodes, and also limits visualisation of the technique by the patient. The position of the couch in the room was arranged according to the position of the lesion in the breast and whether the right or left breast required a biopsy. The couch could not always be placed in the room with sufficient space around it for the practitioners to work in a safe and uncluttered environment. The specimen cabinet was installed in a larger room used for conventional stereotactic biopsies. This meant that the core specimens had to be carried through the centre to be Xrayed in the specimen cabinet before the procedure could be completed. Very often, the biopsy practitioner left the X-ray room in order to view the specimen radiograph, which added to delay in the procedure when it occurred. Coarse calcification, masses and distortions were well visualised, with distortions being particularly well seen. It was easy to identify spiculations and the centre of the lesion could be targeted with ease. For faint calcifications which are difficult to see on standard 2D images, the tomosynthesis images did not improve the visualisation of the area. This was in keeping with the results found during the evaluation of the Hologic Selenia Dimensions tomosynthesis system where calcifications were seen equally well with tomosynthesis and in 2D images. As a result, practitioners tended to avoid biopsying faint calcifications with the Affirm system. They preferred to use the standard 2D equipment which was already in use in the centre. Alternatively, the Affirm could have been used in 2D mode for these cases, but this was not part of the current evaluation. On occasions radiologists asked for additional views during the procedure, and the less experienced radiographers then had to seek advice from more experienced colleagues on how to take these views. Because of rotation between the centre and the vans, many had few occasions to carry out the procedure and long intervals between such occasions. In retrospect, it was too ambitious to try to give all radiographers an opportunity to experience the system. It would have been better to have trained four or five super-users, who would then have cascaded information to the others. An instruction sheet developed in-house might have helped to prompt those who used the system infrequently. None was developed for this evaluation, but several staff expressed a wish for such a document. Some of the radiographers’ comments, for example, a perceived difficulty in attaching the Affirm to the Selenia Dimensions, are attributable to those individuals who had had limited experience with the equipment. A number of factors caused some inconvenience to the radiographers during the evaluation. The location and size of the X-ray room (small and out of the main clinical area) and the specimen cabinet (in another room where the majority of 2D stereotactic biopsies are taken), in particular, seemed to colour the overall perceptions of some respondents. These limitations of the evaluation setup were not at all related to the Affirm or the tomosynthesis biopsy procedure. Some radiographers made a number of comments on the fitting and removing of the stereotactic equipment and the needle guide which were not related to the equipment itself, but rather to the experience which come through usage of the equipment. Similarly, the comments radiographers made about cleaning the stereotactic equipment with wipes instead of by immersion in cleaning solution were mainly a reflection of this procedure being different from what they are used to in the centre. Issues with possible contamination of the touchscreen were also the result of the way practitioners operate in the centre. They usually change the needle position themselves rather than having a nurse or radiographer do it. The screen is therefore covered with cling film during use, to prevent contamination. In particular, the upgrade with the Multi-Pass system was seen as an important improvement on the previous software version. Conclusions and recommendations the Hologic Affirm tomosynthesis biopsy system was found to be useful and effective, particularly for distortions and for masses not seen on ultrasound. Positive feedback was given by the clinicians and the advanced practitioners who carried out biopsy procedures. The opinions of radiographers were more mixed, with generally more positive comments made by those who had assisted with more than two or three biopsies. The equipment performed well over the evaluation period, with only a few technical faults which were resolved. Measurements indicated a significant dose saving for tomosynthesis biopsy compared with stereotactic biopsy. Quality Assurance guidelines for mammography: Including radiographic quality control. Guidance notes for equipment evaluation and protocol for user evaluation of imaging equipment for mammographic screening and assessment. Practical evaluation of Hologic Selenia Dimensions digital breast tomosynthesis system. Technical evaluation of Hologic Selenia Dimensions 2-D digital breast imaging system with software version 1. Evaluation and clinical assessment of the Hologic Selenia Dimensions full field direct digital mammography unit. Routine quality control tests for full field digital mammography systems, 4th Edition. Core needle biopsy and general questions Comments and observations How do you rate the supplier’s operator manual (if used)? I was taught by my colleagues Too many staff to get through the training How do you rate the ease of use of the equipment for tomosynthesis core needle biopsy? We used cling film to keep it clean I don’t feel we are cleaning it as well as for normal stereo equipment. We cannot soak in a chemical cleaner to kill off any blood – can only use Clinell wipes Cleaning with Clinell wipes only. The hubs are disposable How do you rate the ease of rotation of the support arm with the stereotactic equipment fitted and the ease of angulation of X-ray tube assembly? Compression is tolerated Seems very acceptable to all the women I have been involved with Seems comparable to standard stereo How do you rate the image quality of tomosynthesis images for biopsy at the acquisition workstation? Should have the cabinet close by in the same room Better in same room What was your level of confidence in the system for tomosynthesis core needle biopsy? Long gaps between use meant I lost confidence Lack of training and not enough practice and never observed a biopsy taking place, so confidence low when actually had to assist in performing one. Lucky that the doctor was an advanced practitioner and had experience of radiography side Very little exposure to equipment, so very good considering limited experience Not experienced enough yet Like the new software Average for calcium with what I have seen Were there any potential hazards during tomosynthesis core needle biopsy to: a. Does not seem as good as conventional for calcium Sure it will be fine, just need more practice For distortion excellent. Good and quick for radiographers, but more training needed Does not seem very accurate for calcs Less familiar, therefore appears more difficult room too small Poor for calcs Any additional comments on tomosynthesis core needle biopsies Software upgrade to 1. Vacuum biopsies Comments and Observations How do you rate the supplier’s operator manual (if used)? Comment on the accuracy of positioning the vacuum equipment with tomosynthesis 8 N/A, 3 good, 2 average, 2 satisfactory Same as 3D without vacuum 57 Practical evaluation of Hologic Affirm breast tomosynthesis biopsy system Were the compression times acceptable for tomosynthesis vacuum biopsy? Interested to see results of histology compared with 3 D Never seen or done one Not enough knowledge to answer. I am uninformed Have not done any so can’t comment Never used Not seen yet 58 Practical evaluation of Hologic Affirm breast tomosynthesis biopsy system Appendix 5: Radiologists’ and advanced practitioners’ answers to questionnaire Table A5. Core needle biopsy and general questions Comments and Observations How good were the operator manual instructions for tomosynthesis biopsy? Space between tube head and biopsy core device and needle holder means that core gun can be rotated through 90º to take samples 59 Practical evaluation of Hologic Affirm breast tomosynthesis biopsy system How do you rate the use of the display screen of the biopsy control module (touchscreen) for targeting and selecting needle sizes in tomosynthesis core needle biopsy? For calcium very poor and not reliable 60 Practical evaluation of Hologic Affirm breast tomosynthesis biopsy system What is your opinion of the following aspects of image quality when using tomosynthesis images for performing core needle biopsies: a. Not so good for fine calcium (poor) As good as – but not necessarily better Any additional comments on 61 Practical evaluation of Hologic Affirm breast tomosynthesis biopsy system tomosynthesis core needle biopsies the new software helps very much in targeting lesions – much more user friendly Table A5. Vacuum biopsy Comments and Observations How good was the applications training provided by the supplier for tomosynthesis vacuum biopsy 2 N/A, 4 excellent, 1 good How easy was it to use the equipment for directing the tomosynthesis vacuum biopsy? Good patient feedback, two patients who had initial conventional stereo biopsies found vacuum less painful/uncomfortable although they had more bruises May be helpful for nursing staff to comment on their increased role to support 62. This is the second article in a series on breast disorders with an emphasis on diagnosis and management in the general practice setting. This article provides an overview of the investigation of patients with a breast symptom and discusses the assessment and management of benign breast lesions including localised nodularity, fibroadenomas and breast cysts. For many women, a great deal of anxiety is have a significant clinical finding such as Fibroadenoma associated with experiencing a breast change. Nodularity in young women2 A fibroadenoma is a focal area of change in the affecting up to one in 11 Australian women in1 (<30 years) that is symmetrical and cyclical, breast tissue that occurs due to overgrowth their lifetime, the majority of breast lumps are may be managed with clinical surveillance of benign breast elements, both stroma and benign. Fibroadenomas account for about is to exclude cancer, provide an explanation of Investigation may be performed if the 12% of all symptomatic breast masses. They3 the nature of the condition, and educate and lump has changed on review, or if at initial have a peak incidence in the 21–25 years age reassure the patient. The cause of fibroadenomas4 Localised nodularity Nodularity or thickening that is is unknown, however, hormonal factors are Localised nodularity is a common finding in asymmetric, or is a new finding in older thought to be important as fibroadenomas are patients who present complaining of a ‘lump’. It is generally considered, even in the presence of normal palpable or impalpable. Nodularity is usually a physiological Biopsy or referral to a breast surgeon palpable fibroadenomas, they are increasingly change. However, a small but important is warranted where clinical findings are involved in investigating and managing proportion of breast cancers may present as suspicious of malignancy. Close clinical follow up is an important part up on imaging performed for other reasons. These changes can then not generally painful, they may be tender, biopsy – is essential for all women who be further evaluated. They are very common and (causing a lump or significant discomfort) can Fibroadenomas vary in their imaging appearance can occur in women of any age, with a peak be offered aspiration for symptomatic relief, and are often not seen on mammography incidence in the 30–50 years age group. A as they may have the same density as the Approximately 7% of women will present with palpable lump that has the features typical of surrounding breast parenchyma. On ultrasound, a fibroadenoma or the amount of fluid secreted exceeds the echoes, thick walls, or an irregular margin), may appear as a well circumscribed, amount absorbed, fluid accumulates causing even if asymptomatic, may require aspiration. Cysts can be single or multiple and Aspiration is considered when a possible with edge shadowing; gentle lobulations may appear to be hormonally responsive, often cystic lesion cannot be distinguished from be present. They tend to disappear after menopause, aspiration is usually performed under although they can persist or occur de novo in ultrasound guidance and a sample of Differential diagnoses postmenopausal women on hormone therapy. Cysts that are apparent and imaging features as a fibroadenoma, clinically, classically present as lumps that are Fluid from cysts that are aspirated to relieve may be benign or malignant, and are always smooth, soft to firm, mobile, and sometimes symptoms do not need to be sent for managed with surgical excision tender.
For palatal swellings which are suspected salivary tumours treatment 5 of chemo was tuff but made it cheap chloroquine 250 mg amex, incisional biopsies Lynch and Morris treatment viral conjunctivitis buy genuine chloroquine line. This is due to the anatomy of the using a suture during an incisional biopsy region as lesions can be a considerable would also produce minimal artefacts medications given during labor order chloroquine canada. Orientation of biopsies depth beneath the mucosa and so a superfiA case has been reported of surgical the majority of mucosal biopsies are incicial biopsy may give a false negative result medications ritalin buy chloroquine without a prescription. Incisional biopsies should never be punch biopsies does require the receiving If malignancy is suspected symptoms 4 months pregnant 250 mg chloroquine for sale, the biopsy performed treatment type 2 diabetes purchase chloroquine mastercard. Smaller lesions obviously withlaboratory to be familiar with the handling should be of sufficient depth and have a in the soft tissues can safely be excised. If in doubt, contact the surrounding margin to ensure adequate Larger lesions, particularly those affecting laboratory prior to performing the biopsy. In case the lesion was not comthe lip are best ablated with either laser or Also, it is generally safer to use the larger pletely excised it should be orientated. The disadvantage of these diameter punches to avoid handling probthis can be achieved by placing a suture techniques is the lack of material for histolems both clinically and in the laboratory. These techniques are biopsy an adequate depth of tissue should A technique new to the oral cavity but specialised and the reader is directed be obtained to include the epithelium and a established for other bodily sites is that of towards other publications for details of few millimetres of underlying lamina prothe brush biopsy. Traditional incisional biopsies are in fine needle aspiration biopsy and exfoliamer is often best performed by or under the the shape of an ellipse, the length of which tive cytology, this technique uses a small guidance of an experienced cytologist. Description of the clinical appearance of the lesion and suspected diagnosis electrosurgical or laser cutting of tissue. The relationship of the lesion to restorations, particularly amalgam tissue, a zone of thermal necrosis and a zone of tissue exhibiting thermal damage 5. Smoking and alcohol consumption cutting should not be used for diagnostic incisional biopsies. The fixative which is capable of being secured by adhegested that punch biopsies can be left should be 10% neutral buffered formalin sive tape. The traditional use Occasionally, formalin is further diluted tainers are available for this purpose. Formalin fixes the name and address of the sender should the supply of catgut (manufactured from specimens by forming intermolecular be clearly displayed. Where ing produced by formalin is that the specian acceptable alternative; again this will large palatal biopsies are planned, the men is rendered unsuitable for immunofluorequire some pre-arrangement. The diagnosis of for cytogenetics may be required to conneath a denture or pre-constructed acrylic vesiculobullous autoimmune disorders is firm genetic changes in rare tumours (for base plate can be helpful. A regional block can also be than one specimen has to be placed in the examine surgical margins perioperatively. Sampling of tissues at the site means of sutures; do not rely on describcontainer or petri-dish. Prior to taking the of the local anaesthetic will produce arteing the shapes of the pieces of tissue subspecimen at operation, it is both advisable factual tissue oedema or distortion. For mitted because when they are fixed this and courteous to telephone the laboratory to example bulla formation in gingival tissue will probably have altered. For mucosal ensure technical support and a pathologist or oedema which may lead to confusion in disease it is desirable for the pathologist are available. Accompanying information such logical specimens through the post to the ma is one of the diagnostic features. Both the tissue and the formalin the biopsy should be planned before local interpretation of the specimen, in turn, in which it is placed are potentially harmful anaesthetic is administered. Major vessels producing a more meaningful and useful to those handling the specimen. Most of the regulations are common palate, incisions should run parallel to the provide a useful and meaningful diagnosis. Paper towels or diagnosis or even render the specimen It is advised that all patients give cotton wool are suitable for this purpose. It would be appropriate to in a non-diagnostic biopsy and may complication of punch biopsy. Oral Diseases1998;4: include on the consent form the indication necessitate the patient having a repeat 41-42. Improving detection of precancerous and can be induced in the lips or the tongue, 1. Removal of mucoendodontic periradicular surgical specimens-is it cutting biopsy of lesions of the head and neck. Edinburgh: Churchill Livingstone, 1980: experience following oral mucosal biop644-645. J Oral Maxillofac Surg1985; give the standard post-operative oral sur29:303-307. Krause L S, Cobb C M, Rapley J W, Kilroy W J, Spencer pathology of oral cancer and precancer. For further information about submitting your paper electronically please e-mail: k. With that diagnosis, your life has changed and the days ahead will bring more changes and challenges. The doctors, nurses and other experienced health professionals at the University of Michigan Breast Care Center created this handbook to help explain the different surgical treatment options available to you as well as explain how to prepare for surgery and what to expect after surgery. Your medical team is available to help answer questions about this material and to help you decide which treatment options are right for you and give you the best chances of controlling your cancer. Remember that medical knowledge concerning breast cancer treatment options is always advancing, so we will update you on the newest treatment options available. Because of advances in breast cancer detection and management, most patients will be treated successfully! As you have just received a cancer diagnosis and are reading through this handbook, you’re likely feeling overwhelmed. If so, you’re not alone – most patients and family members feel that way as they are introduced to the new concepts, tools, techniques and resources involved in cancer treatment. The information in this handbook will be reviewed and discussed throughout your treatment. You will find blank pages at the back of the handbook to use for questions, appointments or other notes. Through the portal you may securely access health information anywhere, at any time. With the portal you can message your care team, request appointments and prescription refills, pay your bill and more. Each patient receives the benefit of input from several experts in breast cancer care. Most patients with invasive breast cancer who are candidates for surgery will be scheduled for an initial full-day Monday clinic visit. We encourage you to bring one support person, be it a spouse, significant other, relative or close friend. In the morning, you will undergo a complete clinical evaluation (history and physical examination) as well as breast imaging consultation (which often involves repeat/updated mammography and/or breast ultrasound). In the afternoon, you’ll return to the clinic rooms where you will meet with one or more breast specialists to finalize your management plan. We know this is a busy day, but it does cut down on multiple visits to consult with different specialists who are involved with your treatment plan. In addition, it ensures that all members of the treatment team are working in a coordinated way. If you require evaluation for cancer genetic profiling, you will need to schedule a separate consultation appointment with the breast oncology medical genetics specialists. Your treatment team will discuss whether this genetic profiling information is recommended for your care. Many breast cancer patients receive multimodality care (surgery, medical treatment/chemotherapy, radiation) and often the results of one component of care will influence the plan for the subsequent type of care. Follow-up evaluations usually involve shorter visits, depending upon the complexity of your individual case. While discussing many aspects of multidisciplinary breast cancer treatment, this guide focuses on the surgical component of your care. Your breast surgery may be performed at University Hospital, East Ann Arbor Ambulatory Surgical Unit or at some other surgical facility within the University of Michigan Health System. Where your surgery is performed will depend upon the resources that are necessary for your particular operation and surgical suite availability. Some procedures require the combined services of a surgical breast oncologist, breast radiologist and/or the plastic/reconstruction surgeon. Some operations involve the use of pathology assessments during the surgery itself. Your options will be discussed with you by your treatment team and reviewed when a final plan is decided. You may have a preoperative (before surgery) visit at a University of Michigan’s Preoperative Clinic. At this visit you will have a physical examination, review your surgical plan and sign an informed consent document. On the day of your surgery, you will have a final brief preoperative conversation with your surgical and anesthesia team. Your surgery incision and postoperative (after surgery) care may vary depending on your surgeon’s preferences, and she/he will discuss this with you on the day of your surgery. The final results/pathology report from your surgical procedure will be available in two to five business days. If you have undergone plastic/reconstruction surgery, you will have separate postoperative visits with your plastic surgery team. We understand your desire to have as much information as quickly as possible regarding the status of your breast cancer and recommended treatment plan. Please understand that our goal is to obtain a comprehensive assessment that enables us to develop the best possible treatment options for your individual situation. The breast is made up of lobules, which are milk glands that produce the milk, and ducts, which carry the milk from the lobule to the nipple during lactation (when milk is being produced). The ducts and lobules are connected like branches on a tree trunk, forming a closed system of thousands of microscopic channels and tubules that extend throughout the breast. A malignancy (cancer) involving cancerous cells that are confined to the microscopic ductal and/or lobular structures is called in situ or non-invasive breast cancer. When the cancer cells have disrupted the microscopic boundaries of the ductal and lobular channels, it is called invasive or infiltrating breast cancer. A breast biopsy involves taking a sample of breast tissue and having it analyzed under a microscope by a specially trained doctor called a pathologist. The pathologist then provides a report about whether the sampled breast tissue is benign (non-cancerous) or malignant (cancerous). If the biopsy reveals cancer, then the pathologist also describes the pattern of the cancer and whether it is in-situ/non-invasive, invasive/infiltrating or a combination of both. In addition to many thousands of microscopic ductal and lobular units, the breast is also comprised of fatty tissue, blood vessels and other drainage channels called lymphatic vessels (See Figure 1). Invasive breast cancers are capable of extending into these vascular and lymphatic drainage channels, with the potential for spreading to other organs of the body. Extension of a cancer into other organs beyond the breast is called metastatic spread. The nipple is centered in the areola, a dark area of skin in the middle of the breast. A thick muscle (the pectoralis muscle, or pec ) lies underneath the breast, covering the ribs. It drains, or filters, the tissue of the breast, then passes through the lymph nodes, where it is filtered again, then travels back into the blood stream. They are located on both sides of your chest bone (internal mammary chain), under your arms (axillary chain) and above your collarbone (supraclavicular chain). Most of the breast is drained into the axillary lymph node chain under the arm, but occasionally they drain to the other chains of lymph nodes. Here it is filtered for bacteria, cellular waste, and viruses before it can reach the bloodstream. The presence of cancer cells in lymph nodes is an indication that the cancer has the ability to spread and is a more aggressive type of breast cancer. For this reason, examining the lymph nodes draining the breast in the armpit for breast cancer is an important step in the evaluation of breast cancer. In addition to evaluating the lymph nodes, we also look for clues regarding the aggressiveness of the cancer by studying the size and microscopic pattern of the tumor. Some patients will be candidates for an analysis of the genetic content of their cancer. All of these clues help us develop a treatment plan designed to minimize the life-threatening risk of breast cancer for each individual patient. As a result of these improvements, the majority of patients will be cancer-free, long-term survivors. Men at any age may develop breast cancer, but it is usually found in men between 60 and 70 years of age. Male breast cancer makes up less than one percent of all cases of breast cancer in the United States. Invasive/Infiltrating ductal carcinoma: Cancer that has spread beyond the cells lining ducts in the breast. Survival for men with breast cancer is similar to that for women with breast cancer when their stage at diagnosis is the same.
The overall specificity of assessing smoking habits can be increased by supplementing the carbon monoxide data with other measurements (such as self-report and serum cotinine level) that are not affected by air pollution medicine to stop diarrhea cheap chloroquine online. A study of stress as an antecedent to myocardial infarction medications quizlet discount 250mg chloroquine with visa, for example medicine over the counter order chloroquine 250mg on line, would need to consider which kind of stress (psychological or physical treatment 1st degree heart block purchase generic chloroquine line, acute or chronic) was of interest before setting out the operational definitions for measuring it symptoms 1dp5dt purchase chloroquine overnight delivery. Measurements should provide an adequate distribution of responses in the study population medications identification order chloroquine with visa. A measure of functional status is most useful if it produces values that range from high in some subjects to low in others. One of the main functions of 46 Basic Ingredients pretesting is to ensure that the actual responses do not all cluster around one end of the possible range of response (Chapter 17). This is achieved by reducing the involvement of the observer and by increasing the structure of the instrument. The danger in these strategies, however, is the consequent tunnel vision that limits the scope of the observations and the ability to discover unanticipated phenomena. The best design is often a compromise, including an opportunity for acquiring subjective and qualitative data in addition to the main objective and quantitative measurements. Some of these measurements can only be made during a contact with the study subject, but many can be carried out later on biological specimens banked for chemical or genetic analysis, or on images from radiographic and other procedures filed electronically. One advantage of such storage is the opportunity to reduce the cost of the study by making measurements only on individuals who turn out during follow-up to develop the condition of interest. A terrific approach to doing this is the nested case–control design (Chapter 7); paired blinded measurements can be made in a single analytic batch, eliminating the batch-to-batch component of random error. A second advantage is that scientific advances may lead to new ideas and measurement techniques that can be employed years after the study is completed. The growing interest in translational research (Chapter 2) takes advantage of new measurements that have greatly expanded clinical research in the areas of genetic and molecular epidemiology (4,5). Measurements on serum can be used to study molecular causes or consequences of disease; for example, proteomic patterns may provide useful information for diagnosing certain diseases (6). It is important to consult with experts regarding the proper collection tubes and storage conditions in order to preserve the quality of the specimens and make them available for the widest spectrum of subsequent use. In Chapter 9 we will address the issue of choosing measurements that will facilitate inferences about confounding and causality. And in Chapter 15 we will address the topic of questionnaires and other instruments for measuring information supplied by the study subject. In designing measurements it is important to keep in mind the value of efficiency and parsimony. The full set of measurements should collect useful data at an affordable cost in time and money. Efficiency can be improved by increasing the quality of each item and by reducing the number of items measured. Collecting more data than are needed is a common error that can tire subjects, overwhelm the research team, and clutter data management and analysis. The result may be a more expensive study that paradoxically is less successful in answering the main research questions. Variables are either continuous (quantified on an infinite scale), discrete (quantified on a finite scale of integers), or categorical (classified in categories). Categorical variables are further classified as nominal (unordered) or ordinal (ordered); those that have only two categories are termed dichotomous. Clinical investigators prefer variables that contain more information and thereby provide greater power and/or smaller sample sizes: continuous variables > discrete variables > ordered categorical variables > nominal and dichotomous variables. Precision is reduced by random error (chance) from three sources of variability: the observer, the subject, and the instrument. Strategies for increasing precision that should be part of every study are to operationally define and standardize methods in an operations manual, and to train and certify observers. Other strategies that are often useful are refining the instruments, automating the instruments, and using the mean of repeated measurements. The strategies for increasing accuracy include all those listed for precision with the exception of repetition. In addition, accuracy is enhanced by unobtrusive measures, by calibration, and (in comparisons between groups) by blinding. Individual measurements should be sensitive, specific, appropriate, and objective, and they should produce a range of values. In the aggregate, they should be broad but parsimonious, serving the research question at moderate cost in time and money. Investigators should consider storing banks of materials for later measurements that can take advantage of new technologies and the efficiency of nested case–control designs. This example, from the operations manual of the Study of Osteoporotic Fractures, describes the use of a dynamometer to measure grip strength. To standardize instructions from examiner to examiner and from subject to subject, the protocol includes a script of instructions to be read to the participant verbatim. Protocol for Measuring Grip Strength with the Dynamometer Grip strength will be measured in both hands. The handle should be adjusted so that the participant holds the dynamometer comfortably. The participant’s arm should be flexed 90 at the elbow with the forearm parallel to the floor. While demonstrating, use the following description: ‘‘This device measures your arm and upper body strength. Allow one practice trial for each arm, starting with the right if she is right handed. On the second trial, record the kilograms of force from the dial to the nearest 0. The gripping action should be a slow, sustained squeeze rather than an explosive jerk. Hulley After an investigator has decided whom and what she is going to study and the design to be used, she must decide how many subjects to sample. Even the most rigorously executed study may fail to answer its research question if the sample size is too small. On the other hand, a study with too large a sample will be more difficult and costly than necessary. The goal of sample size planning is to estimate an appropriate number of subjects for a given study design. Although a useful guide, sample size calculations give a deceptive impression of statistical objectivity. They are only as accurate as the data and estimates on which they are based, which are often just informed guesses. It often reveals that the research design is not feasible or that different predictor or outcome variables are needed. Therefore, sample size should be estimated early in the design phase of a study, when major changes are still possible. Before setting out the specific approaches to calculating sample size for several common research designs in Chapter 6, we will spend some time considering the underlying principles. Readers who find some of these principles confusing will enjoy discovering that sample size planning does not require their total mastery. However, just as a recipe makes more sense if the cook is somewhat familiar with the ingredients, sample size calculations are easier if the investigator is acquainted with the basic concepts. Hypotheses are not needed in descriptive studies, which describe how characteristics are distributed in a population, such as a study of the prevalence of a particular genotype among patients with hip fractures. Hypotheses are needed for studies that will use tests of statistical significance to compare findings among groups, such as a study of whether that particular genotype is more common among patients with hip fractures than among controls. Because most observational studies and all experiments address research questions that involve making comparisons, most studies need to specify at least one hypothesis. If any of the following terms appear in the research question, then the study is not simply descriptive, and a hypothesis should be formulated: greater than, less than, causes, leads to , compared with, more likely than, associated with, related to , similar to , correlated with. Characteristics of a Good Hypothesis A good hypothesis must be based on a good research question. A simple hypothesis contains one predictor and one outcome variable: A sedentary lifestyle is associated with an increased risk of proteinuria in patients with diabetes A complex hypothesis contains more than one predictor variable: A sedentary lifestyle and alcohol consumption are associated with an increased risk of proteinuria in patients with diabetes Or more than one outcome variable: Alcohol consumption is associated with an increased risk of proteinuria and of neuropathy in patients with diabetes Complex hypotheses like these are not readily tested with a single statistical test and are more easily approached as two or more simple hypotheses. Sometimes, however, a combined predictor or outcome variable can be used: Alcohol consumption is associated with an increased risk of developing a microvascular complication of diabetes. In this example the investigator has decided that what matters is whether a participant has a complication, not what type of complication occurs. A specific hypothesis leaves no ambiguity about the subjects and variables or about how the test of statistical significance will be applied. It uses concise operational definitions that summarize the nature and source of the subjects and how variables will be measured. Use of tricyclic antidepressant medications, assessed with pharmacy records, is more common in patients hospitalized with an admission diagnosis of myocardial infarction at Longview Hospital in the past year than in controls hospitalized for pneumonia. Chapter 5 Getting Ready to Estimate Sample Size: Hypotheses and Underlying Principles 53 this is a long sentence, but it communicates the nature of the study in a clear way that minimizes any opportunity for testing something a little different once the study findings have been examined. It would be incorrect to substitute, during the analysis phase of the study, a different measurement of the predictor, such as the self-reported use of pills for depression, without considering the issue of multiple hypothesis testing (a topic we discuss at the end of the chapter). Usually, to keep the research hypothesis concise, some of these details are made explicit in the study plan rather than being stated in the research hypothesis. But they should always be clear in the investigator’s conception of the study, and spelled out in the protocol. It is often obvious from the research hypothesis whether the predictor variable and the outcome variable are dichotomous, continuous, or categorical. If it is not clear, then the type of variables can be specified: Alcohol consumption (in mg/day) is associated with an increased risk of proteinuria (>300 mg/day) in patients with diabetes. If the research hypothesis begins to get too cumbersome, the definitions can be left out, as long as they are clarified elsewhere in the protocol. Most important, this will keep the research effort focused on the primary objective. A single prestated hypothesis also creates a stronger basis for interpreting the study results than several hypotheses that emerge as a result of inspecting the data. Hypotheses that are formulated after examination of the data are a form of multiple hypothesis testing that can lead to overinterpreting the importance of the findings. Types of Hypotheses For the purpose of testing statistical significance, the research hypothesis must be restated in forms that categorize the expected difference between the study groups. Thenull hypothesis states that there is no association between the predictor and outcome variables in the population (there is no difference in the frequency of drinking well water between subjects who develop peptic ulcer disease and those who do not). Assuming that there really is no association in the population, statistical tests help to estimate the probability that an association observed in a study is due to chance. The alternative hypothesis cannot be tested directly; it is accepted by default if the test of statistical significance rejects the null hypothesis (see later). A one-sided hypothesis specifies the direction of the association between the predictor and outcome variables. The hypothesis that drinking well water is more common among subjects who develop peptic ulcers is a one-sided hypothesis. A two-sided hypothesis states only that an association exists; it does not specify the direction. The hypothesis that subjects who develop peptic ulcer disease have a different frequency of drinking well water than those who do not is a two-sided hypothesis. An example is the one-sided hypothesis that a new drug for hypertension is more likely to cause rashes than a placebo; the possibility that the drug causes fewer rashes than the placebo is not usually worth testing (it might be if the drug had anti-inflammatory properties! A one-sided hypothesis may also be appropriate when there is very strong evidence from prior studies that an association is unlikely to occur in one of the two directions, such as a study that tested whether cigarette smoking affects the risk of brain cancer. Because smoking has been associated with an increased risk of many different types of cancers, a one-sided alternative hypothesis. Indeed, in these two examples, the results of well-done trials revealed a statistically significant effect that was opposite in direction from the one supported by previous data (1–3). Overall, we believe that nearly all alternative hypotheses deserve to be two-sided. It is important to keep in mind the difference between a research hypothesis, which is often one-sided, and the alternative hypothesis that is used when planning sample size, which is almost always two-sided. For example, suppose the research hypothesis is that recurrent use of antibiotics during childhood is associated with an increased risk of inflammatory bowel disease. That hypothesis specifies the direction of the anticipated effect, so it is one-sided. Statistical rigor requires the investigator choose between oneand two-sided hypotheses before analyzing the data; switching to a one-sided alternative hypothesis to reduce the P value (see below) is not correct. In addition (and this is probably the real reason that two-sided alternative hypotheses are much more common), most grant and manuscript reviewers expect two-sided hypotheses, and are critical of a one-sided approach. Because an investigator cannot study all middle-aged women with diabetes, she must test the hypothesis in a sample of that target population. In some ways, the investigator’s problem is similar to that faced by a jury judging a defendant (Table 5. The absolute truth about whether the defendant committed the crime cannot usually be determined. Instead, the jury begins by presuming innocence: the defendant did not commit the crime. The jury must decide whether there is sufficient evidence to reject the presumed innocence of the defendant; the standard is known as beyond a reasonable doubt. A jury can err, however, by convicting an innocent defendant or by failing to convict a guilty one. Guilt: the defendant did counterfeit Alternative hypothesis: There is an association between money. Standard for rejecting innocence: Standard for rejecting null hypothesis: Level of Beyond a reasonable doubt.
Our goal was to identify predictors of pathogenic variants and assess indicators for expanded genetic testing symptoms uti generic chloroquine 250 mg amex. Methods: We conducted a retrospective review of breast and ovarian cancer patients who underwent panel testing between May 2011 and April 2016 treatment 4 addiction buy generic chloroquine online. A variety of commercial gene panels were used with variant classification determined by the individual laboratory illness and treatment chloroquine 250mg otc. Results: We identified 215 patients who underwent panel testing: the average age of patients was 52 treatment synonym purchase chloroquine with mastercard. However treatment bipolar disorder order chloroquine, individuals with pathogenic variants tended to have a younger age of first cancer diagnosis medicine nobel prize 2015 discount chloroquine 250 mg on-line, have higher grade disease and have triple negative tumors. Expanded panel testing should be considered in patients with a younger age of cancer diagnosis, higher grade disease and triple negative tumors. Body: Background the identification of individuals at elevated risk for hereditary cancers has allowed the development of consensus recommendations for cancer screening and prevention. Therefore, the multigenerational panel increase the need for genetic counseling suggesting preventive approach or cancer-specific screening to patients and family members. The rapid clinical introduction of multigene panel testing, however, have several issues such as lowto moderate-risk gene mutations and clinical recommendations. We collect the mutation results and clinical recommendations after testing with multigene panel and giving genetic counseling. Methods We had developed multigene panel consisted of 64 genes related to hereditary cancer through previous study and prospectively enrolled 104 individuals who were appropriate candidates for hereditary breast cancer evaluation. The patients were tested with 64-gene panel(Celemics) and results were provided by us 4~10 weeks later. We recommended the cancer-specific screening and/or preventive approach for mutation-positive patients and suggested additional genetic test for the family members. Among them, 6 (23%) patients received Risk reducing procedures (Prophylactic mastectomy or oophorectomy) and most of them(19 patients(73%)) received cancer specific screening. Conclusion We demonstrate the use of multigene panel testing for hereditary breast cancer and will suggest the process of the genetic counseling including indication and results analysis with multigene panel testing. The online survey included items on demographics, breast cancer risk factors, and validated measures of genetic testing intention/knowledge, breast cancer worry/risk perception, stigma, and religious/cultural factors affecting medical decision-making. Descriptive statistics and bivariate and multivariable logistic regression models were conducted. We conducted 4 focus groups with purposive sampling of women who responded to the survey. Results: Among 321 evaluable survey participants, median age was 47 years (range, 25-82); 55. Compared to Modern Orthodox women, non-Modern Orthodox women were more likely to consult with a rabbi or religious figure when considering genetic testing and other medical decisions. The focus group participants (N=31) confirmed the importance of rabbinic consultation in medical decision-making. Although stigma was not associated with genetic testing uptake in our survey data, it emerged as a prominent factor in decision-making among focus group participants due to its potential impact on marriageability and family. Among non-Modern Orthodox women, rabbinic consultation was an important factor in genetic testing decision-making. The majority of patients were of European (66%) or African (31%) American ancestry; 26% had a family history and 13% had died of disease with an average time to death of 2. The opinions or assertions contained herein are the private ones of the author/speaker and are not to be construed as official or reflecting the views of the Department of Defense, the Uniformed Services University of the Health Sciences or any other agency of the U. University Hospital of South Manchester, Manchester, United Kingdom; University of 3 4 Manchester, Manchester, United Kingdom; Karolinska Institute, Stockholm, Sweden; University of Cambridge, Cambridge, 5 United Kingdom and Queen Mary University of London, London, United Kingdom. Body: Background Previous studies have demonstrated that treatment with tamoxifen reduces breast density in a proportion of women. Women at increased familial risk of breast cancer (n=135) aged 33-46 agreed to take tamoxifen for five years for breast cancer prevention. Controls (n=204) were of the same age and risk, undergoing annual mammography in the same clinic. We report response data for each technique related to median change in dense volume or dense area after one year and 4-5 years of tamoxifen treatment. Median density in women taking tamoxifen at baseline and 1 year for V, D and S were 61. The median and interquartile ranges for change in density from baseline to year 1 were 10. This study confirms that tamoxifen produces marked reductions in density measured by automated techniques based on change in dense volume (Volpara), dense area (Densitas and Stratus) which can be used to assess response to tamoxifen in women on an annual mammography programme. However correlations between techniques were relatively low and suggests that more than one technique might be used in practice. Virtually all of the reduction in density seen at one year was sustained for as long as treatment continued. Whether the marked rise in density after early cessation of tamoxifen seen in some women is detrimental remains to be investigated. In summary, we demonstrate that change in density as a result of tamoxifen treatment may be evaluated by automated techniques which may be more applicable than visual techniques in the clinic. Institute of Genetics and Molecular 2 Medicine, University of Edinburgh, Edinburgh, United Kingdom and Edinburgh Breast Unit, Western General Hospital, Edinburgh, United Kingdom. Cytoplasmic/membrane staining was scored using a graduated scale (0-3+) and nuclear staining was graded using an Immunoscore. The full-length membrane bound molecule comprises 8 domains: 6 extracellular, 1 transmembrane and 1 cytoplasmic. Lower levels were associated with increased energy generation, cellular metabolism and epithelial-mesenchymal transition. The aim was to validate this test in cohorts of both preand post-menopausal women treated with two weeks of a variety of endocrine treatments (tamoxifen, fulvestrant or an aromatase inhibitor) prior to surgery. The 5 and 10 year actuarial recurrence rates were 7%/22% and 46%/73% for the low and high risk groups, respectively. The actuarial breast cancer-related death rate for the low risk group was 5% at both 5 and 10 years, whereas for the high risk group was 33%/38%. The 5 and 10 year actuarial recurrence rates were 12%/29% and 27%/77% for the low and high risk groups, respectively. The 5 and 10 year actuarial breast cancer-related death rates were 7%/19% and 9%/58% for low and high risk groups, respectively. As a result, the cost effective role of clinical risk assessment with histopathology of breast carcinomas tends to be minimized. Patients had five years of follow-up with tumor registry and were treated with endocrine therapy alone. Results Patient ages were 33-92, with mean/median age of 60, and all had endocrine therapy alone. Estrogen receptor H Score/Allred Score was strong (Allred Score 7-8) in 395/441 (89. At 5 years, 433 patients (98%) were alive, 8 were dead, 1 from breast cancer due to distant recurrence. Body: Background Polymorphisms of genes involved in estrogen production have been linked to breast cancer risk, prognosis and treatment response. Exemestane showed a significant 10% absolute reduction in Ki67 labeling index compared to the other two arms. Serum and whole blood was taken at baseline and the day before surgery and stored at -80°C until assayed. The association of genetic polymorphisms with any event was assessed by the Cox proportional hazards models adjusted for confounders. Results the genetic polymorphisms did not deviate from Hardy-Weinberg equilibrium (P-value >0. Interestingly, the carriers of the variants associated with lower estrogen levels at diagnosis had better prognosis. Further genomic profiling in larger trials aimed to enhance tailored treatment efficacy in endocrine-responsive postmenopausal breast cancer are warranted. These results were supported by Western blots from the cell lines examined under various growth conditions. This combination might be an interesting treatment option for tamoxifen-resistant patients. Hokkaido University Hospital, Sapporo, Hokkaido, Japan; Hokkaido University Hospital, Sapporo, Hokkaido, 3 Japan and Research Division of Companion Diagnostics, Hokkaido University Hospital, Sapporo, Hokkaido, Japan. We recently reported that approximately two-thirds of patients who relapsed within 5 years had received anthracyclins and/or taxanes as adjuvant or neoadjuvant chemotherapy in addition to adjuvant endocrine therapy. New strategies, such as signal transduction inhibitors together with endocrine therapy are required to improve survival. Correlations between these biological markers and clinicopathological factors and prognosis were analyzed separately in preand postmenopausal women. A long follow up retrospective study 1 1 1 1 1 1 1 1 Miguel Gil-Gil, Idoia Morilla, Anna Petit, Teresa Soler, Xavier Perez-Martin, Anna Guma, Maria Jesus Pla, Raul Ortega, 1 1 1,2 1 1 1 1 Amparo Garcia-Tejedor, Catalina Falo, Robert Montal, Luis Perez-Casanova, Carolina Loayza and Sonia Pernas. Surgical specimen: ypT1 36%, ypT2 54%, ypT3 6%, ypT4 4%; ypN0 28%, ypN1 22%, ypN2 13. However, the potential of this endpoint for predicting the adjuvant efficacy of therapeutic agents remains highly uncertain, motivating continued study based on clinical data. After curating relevant data from multiple trials (in both the neoadjuvant and adjuvant settings), a statistical model was constructed to evaluate the current evidence regarding this hypothesis. Using neoadjuvant Ki67 data for several therapies for which adjuvant data are presently unavailable, we demonstrated how forecasts (and associated confidence intervals) of adjuvant effect-size may be produced using the model. This analysis suggests the potential utility of Ki67 as a surrogate endpoint to screen/prioritize experimental regimens for development in the adjuvant setting. Institut Curie, Paris, France; Versailles Saint 3 Quentin University, Paris Saclay University, Saint Cloud, France and Paris Descartes University, Sorbonne Paris Cite University, Paris, France. Irradiation volumes (breast or chest wall +/regional lymph nodes) were defined per standard of care. Locoregional relapse was defined as documented ipsilateral invasive relapse occurring in the breast, chest wall and/or in regional lymph nodes, prior to any distant metastatic relapse. Cumulative incidence rates and hazard ratio were obtained using both Cox and Fine-Gray models, taking into account metastatic relapse and death as competitive events. Similar results were obtained when taking locoregional relapses synchronous with distant metastatic disease into account (interaction test: p=0. Moreover, the finding that cM0(i+) status is a predictive marker for the efficacy of locoregional lymph node irradiation promises a new opportunity to better tailor adjuvant radiation therapy in early stage breast cancer patients. Lund University, Lund, Sweden; Lund University Cancer Center, Medicon Village, Lund, Sweden; 3 4 5 Skåne University Hospital, Lund, Sweden; Blekinge County Hospital, Karlskrona, Sweden; Skåne University Hospital, Malmö, 6 7 8 Sweden; Skåne University Hospital, Malmö, Sweden; Skåne University Hospital, Lund, Sweden; Lund University, Lund, 9 Sweden and Skåne University Hospital, Lund, Sweden. For 405 breast tumors in the training cohort, a comprehensive histopathological biomarker evaluation was performed by three pathology readings to estimate inter-pathologist variability on the original diagnostic slides as well as on repeat immunostains for this study, and the consensus biomarker status for all five conventional biomarkers was determined. All patients underwent upfront breast surgery; hence there are no confounding effects of neoadjuvant treatment on biomarker levels. Application of the optimal cut point from Cohort A to tumors in the validation Cohort B classified 145/316 cores (45. Results: There were 56 patients in the paclitaxel arm (A), 115 in the Paclitaxel+Neratinib arm (B), 22 patients on the Paclitaxel + Trastuzumab arm (C) and 72 on the Paclitaxel + Veliparib + Carboplatin arm (D). Lund University, Clinical Sciences Lund, Oncology and Pathology, Lund, Sweden; Skåne 3 4 University Hospital, Lund, Sweden; Lund University, Computational Biology and Biological Physics, Lund, Sweden; Uppsala 5 6 University, Uppsala, Sweden; Akademiska University Hospital, Uppsala, Sweden; Karolinska Institutet, Cancer Center 7 8 Karolinska, Stockholm, Sweden; Karolinska University Hospital, Radiumhemmet, Stockholm, Sweden; Skåne University 9 10 Hospital, Lund, Sweden; Karolinska Institutet, Stockholm, Sweden and Karolinska University Hospital, Stockholm, Sweden. Further, genes described in the literature as associated with radioresistance were included in the panel to a total of 248 genes. A custom nCounter (Nanostring Technologies) gene expression panel was designed and both the training and validation cohorts were analyzed with the custom panel. Single-sample classifiers using a k-top scoring pairs algorithm were trained in the training cohort and validated in the validation cohort. The most promising was however that it seems as the panel could be used as a predictive marker, i. Clinicopathologic variables were abstracted from pathology reports, and were available for a subset of these cases. Fudan University Shanghai Cancer Center, Shanghai, China; Cancer Institute, 3 Fudan University Shanghai Cancer Center, Shanghai, China and Shanghai Medical College, Fudan University, Shanghai, China. Training set comprised patients diagnosed between 2003 and 2009, while validation set included patients diagnosed thereafter. Ethical approval of the study was granted by the Institutional Review Board of Fudan University Shanghai Cancer Center. A logistic regression model was used to construct the nomogram in the training set and then validated in the validation set. Nomogram performance was quantified with respect to discrimination and calibration. Larger lesion, younger age at diagnosis, black ethnic and lack of hormone receptor expression were significantly related to regional nodes involvement. A calibration curve for the nomogram was plotted to evaluate the agreement between actual (observed) outcomes and expected probabilities. The slope of the calibration curve was close to 1, which indicated excellent calibration of the nomogram. The nomogram based on the clinical parameters was established, which could accurately predict regional lymph node status. This nomogram would facilitate evaluating lymph node state preoperatively and thus treatment decision-making of individual patients, especially in neoadjuvant settings. Finally, all of these features were combined, evaluated using Ranksum feature ranking, and then used to generate predictive models using four different supervised machine learning classifiers random forest, support vector machine, linear discriminant analysis, and a neural network – via a 3-fold cross validation scheme. Results: the highest performing features were consistently mitosis, epithelial architectural, and tubule features. These features were able to provide the highest level of classification utility for the most distinct cases (L-L vs.
Purchase chloroquine 250mg on line. Child Wheezing | What Does It Mean?.