Deborah W. Wilbur, MD
- Hematologist/Medical Oncologist
- Private Practice
- Oncology Associates
- Cedar Rapids, Iowa
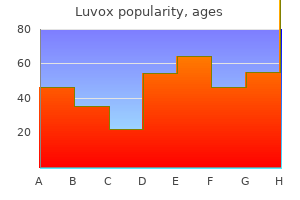
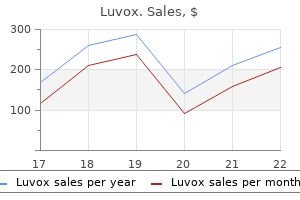
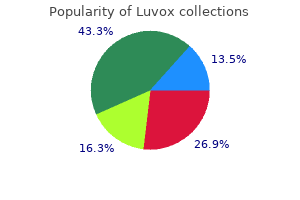
However anxiety guru buy luvox american express, there is a risk that it may increase harms if it is taken by women to be equivalent to a diagnostic test anxiety during pregnancy buy luvox line, if it delays diagnosis for some women (delaying some terminations) and if it makes life more difficult for people with the conditions being screened for anxiety lymph nodes purchase cheapest luvox. This should cover all stages of the pathway and include the provision of accurate anxiety medication 05 mg buy generic luvox canada, balanced and non directive information and support anxiety symptoms 3 year old cheap 50mg luvox free shipping, result giving anxiety symptoms of menopause buy generic luvox 50 mg on line, and dealing with any unanticipated or secondary findings and failed tests. Training should have agreed learning outcomes that cover: the provision of accurate, balanced and non-directive information about the tests and conditions tested for; skills in providing decision-making support and the need for reasonable adjustments to support decision making for those with protected characteristics; and knowledge about the medical and social prospects of people with the conditions being screened for. The training would be enhanced by the involvement of people with different personal experiences of prenatal screening and the conditions being screened for. It is recommended that Public Health England and the fetal anomaly screening programme work with support organisations to deliver these different aspects of training and that this continues as part of a sustainable fetal anomaly screening training programme going forward. Again, the information would be enhanced by the involvement of people with different personal experiences of prenatal screening and the conditions being screened for. Different information resources, in terms of the detail and content of the information, may need to be developed for different points in the pathway and depending on the different conditions being screening for. A skilled health or social care professional should also provide this information verbally and in such a way as to equally support decisions to test and not to test. Women will be asked to decide at this point if they want to have the combined test. Women who receive a high chance result from the combined test should be informed in an appropriate way and be given rapid opportunity to discuss the result with skilled health or social care professionals. Information should be provided in a non-directive way about the implications of the result, the condition(s) for which the high chance result is for, and the options available. A skilled healthcare professional should provide this information verbally and in such a way as to equally support decisions to test or not to test. Women who receive a high chance result should be informed in an appropriate way and given rapid opportunity to discuss the result with skilled health or social care professionals. Information should be provided in a non-directive way about the implications of the result, the condition that has been identified as likely, and the options available. Women who receive a positive result should be informed in an appropriate way and given rapid opportunity to discuss the result with skilled health or social care professionals. Information should be provided in a non-directive way about the implications of the result, the condition that has been detected, and the options available. A skilled healthcare professional should provide this information verbally and in such a way as to equally support decisions to terminate and to continue the pregnancy. In addition, consideration should be given to the social consequences related to any reduction in the number of people with the conditions being screened for; and the potential for sending hurtful or damaging messages to people with the condition and their families. It can provide early, diagnostic information about significant medical conditions or impairments without putting the fetus at risk, giving women the opportunity to prepare psychologically and practically for a disabled child, or to have a termination. In line with international professional guidelines on prenatal testing,376 targeted testing should be used in most cases, and if whole genome or exome sequencing is used, comprehensive patient counselling from qualified health and social care professionals will be essential. Providers should consider the guidance produced by the Human Genetics Commission on the information that should be provided to potential consumers by companies offering genetic testing. The aim of the survey was to gather views from a wide range of individuals, particularly those with personal and professional experiences of prenatal testing and genetic conditions. Survey respondents were self-selecting and the results are not intended to be representative of the views of the population as a whole. The Working Group considered an analysis of the survey responses at its second meeting on 23 September 2016. Comments from some of the survey respondents who consented to being quoted are used in this report but the survey analysis will not be published separately in order to respect the confidentiality of respondents. Call for views and evidence: consultation document Alongside the survey, the Working Group published a consultation document with a longer series of more detailed questions. The consultation was open between 19 May and 1 August 2016, and 28 responses were received. The Working Group considered an analysis of the consultation responses at its third meeting on 24 November 2016 and this will be published separately on the Nuffield Council on Bioethics website. The interviews were conducted by members of the Working Group with counselling experience and took place in October 2016. Dr Barbara Barter, Clinical Psychologist, was recruited to lead the consultation exercise and carry out the interviews. The interviews were preceded by a recruitment process to identify suitable participants carried out with the support of advocacy and campaigning organisations across England. People who were interested in taking part were invited to attend information sessions covering related topics, including sex and relationships, difference and diversity and prenatal screening and termination. A detailed report by Dr Barbara Barter outlining the method and findings of this work has been published separately, at: The interviews were conducted in November and December 2016 by members of the Working Group with counselling experience. One interviewee had spinal muscular atrophy, one had cystic fibrosis and one was a carrier of a balanced translocation genetic variation and had a child with Emanuel syndrome. Dr Gareth Thomas, Lecturer in Sociology School of Social Sciences Cardiff University carried out the review and it has been published separately at It is important, howe ve r, that the person who is thinking about being tested make an info r m e d choice. Fa m i l y, friends and professional support people may also find this material useful in supporting those considering testing. Each person has 23 pairs of chromosomes, half from their father and half from their mother. However, there is a great deal of variability in the symptoms, their severity, and the age of onset, even within the same family. More research is required before accurate risk figures can be given for this range. A person with depression, changes in behavior, or psychiatric illness should also be seen by a psychologist or psychiatrist. The National Society of Genetic Counselors can also provide the name of a genetic counselor in your area. Having a support person, such as a friend or spouse, who is present at all appointments is useful. This person can act, not only as a second set of ears, but also as a sounding board to talk through feelings about testing, and provide support after the test results are given. The decision to be tested is very personal and may be one of the most important decisions you ever face. A person given a normal (negative) 7 result may also feel an increased responsibility to take care of affected family members that he or she may not have felt before testing. How would you tell each of them, for example, by phone, by letter, at a family meeting This is particularly important if you have had problems with depression, anxiety, or thoughts of suicide. Do you plan to tell the people you work with about your decision to be tested or test results Some companies have confidential employee services where you can discuss these concerns. You should be comfortable with your insurance coverage (life, health and disability) before beginning testing. It can be more difficult to deal with the test re s u l t s i f the re s u l t sa re t h e o p p o s i t eo f yo u r i n n e r f e e l i n gs. What things do you do to get out of a slump, for example, call a friend or family member, go for a walk, work out, work in the garden Recognizing what resources have worked for you in the past is helpful because you can start using them again when you need help in the future. It is good to choose a time to be tested when complicating factors from the outside are at a minimum. For example, in the middle of a divorce or break up of a relationship, or at a stressful time at school or work is not a good time to be tested. Testing at a time of celebration may not be optimal, for example, directly before or after marriage, or in the middle of important holidays. It is useful to make a decision about whether or not to be tested even if the decision is not an absolute yes or no answer. Many people feel relief at having an answer and disbelief that the answer is accurate. This is particularly true if those decisions were permanent, for example, decisions about whether or not to have children, or career paths. Feelings such as depression, anger, loss of hope, despair, and severe stress can occur. If these feelings occur, treatment with a psychologist, psychiatrist, or counselor can be very helpful. Most people eventually come to terms with their results and use the information to help make plans for the future. Often there may be a feeling of increased responsibility for caring for affected family members. Sometimes the chorionic villi are removed 13 in a manner similar to amniocentesis. You should consider how you feel about pregnancy termination well in advance of a pregnancy. This is a more costly procedure with a lesser success rate in achieving a pregnancy. A genetic counselor can help individuals and couples identify which options are most compatible with their personal belief systems and life goals. Ideally, you should meet with a genetic counselor prior to considering a pregnancy. Receiving the Huntington Disease Society of American newsletter is an excellent way to stay informed about new advances. Kessler S (1988) Invited essay on the psyc h o l o gi c a l aspects of genetic counseling. Population data were obtained from the database of the Basque Antenatal Screening Programme. Nevertheless, unlike frst and second test are close to 90% [4], non-invasive tests based on trimester screening tests, this approach would not pro genome sequencing and bioinformatics are newly being vide early identifcation of other foetal abnormalities and introduced into clinical practice. Cost Ef Resour Alloc (2019) 17:6 Page 3 of 19 of women undergoing frst and second-trimester screen termination of pregnancies, etc. Diferent ous history of chromosome anomalies, among others), aspects of the prenatal screening. A cost-effectiveness analysis wasdeveloped using real data obtained from the regional Basque AntenatalScreeningProgramme and extrapolating the results to the Spanish National Health Service. Down Syndrome represents an important public health issuegiven that the risk increasesw ith advanced maternal age and older mothers constitute a generaltrend across developed countries. Cost Ef Resour Alloc (2019) 17:6 Page 7 of 19 calculating who would participate in the frst and sec antenatal screening coverage was 78.
With the presence of a congenital brain tumor anxiety in dogs purchase luvox uk, there is an increased frequency of stillbirth; macrocephaly and hydrocephalus are the main present ing signs in the fetus and neonate anxiety hives order luvox canada. Brain tumors in the newborn may present as intracranial hemorrhage anxiety 6 things you can touch with your hands order luvox uk, chronic subdural hematoma anxiety 39 weeks pregnant generic luvox 100 mg otc, neurological decits anxiety care plan cheap luvox 100mg on line, unexplained hydrocephalus anxiety quiz order luvox cheap, or distortion of the cranium with bony defects. In utero some brain tumors grow to an extremely large size and may result in fetal hydrops. Other brain tumors that have been detected prenatally are choroid plexus papilloma, cran iopharyngioma, and astrocytoma (Figures 20. Astrocytomas in the fetus and newborn usually are found outside the cerebellum and above the tentorium cerebelli. Desmoplasticcerebrallarastrocytomatypicallyisfound in infants and appears to be associated with a good prognosis. It is a very aggressive tumor and metastasizes widely within the cerebral spinal uid pathways and may seed to the meninges and the spinal cord. It occurs predominantly in the midline of the cerebellum, the cerebellar hemispheres, pineal body, brainstem, spinal cord or olfactory nerve, and retina. The tumor origi natesfromtheroofofthefourthventricleandcausesobstruction of the cerebral aqueduct and hydrocephalus. Histologically the tu mor consists of small darkly staining cells with variable amounts of intracellular pink-staining material. The cells have round, oval, or carrot-shaped nuclei with coarse chromatin and scant cystoplasm. Ependymoma Ependymomas may occur in the newborn and most arise from the wall of the fourth ventricle (Figure 20. These tumors are responsible for dystocia, stillbirth, and spontaneous intracerebral hemorrhage. Newborns with ependymomas have a poor progno sis; they may recur locally and may disseminate throughout the cerebrospinal uidintotheperitonealcavitybyventricularperitonealshuntcatheterswithout lters. Myxopapillary ependymoma occurs in the region of the chorda equina and has a distinctive papillary appearance. Choriocarcinoma may occur in the newborn from metastatic spread from a maternal choriocarcinoma. We have observed a male infant who died from massive intracranial hemorrhage sec ondary to metastatic choriocarcinoma to the brain, presumably from an unrecognized placental choriocarcinoma. These tumors grow by expansion into the optic chiasm and into the oor of the fourth ventricle and posteriorly into the 20. Microscopic appearance of ependymonas showing characteristic pseudorosette arrangement around blood ves posterior fossa. Although it is a histologically benign tumor, the prognosis may be unfavorable because of its expansile growth. Atypical teratoid/rhabdoid tumor is a highly malignant tumor that may occur in the newborn (Figure 20. It may occur as a solitary tumor or concomitantly with rhabdoid tumor of the kidney or liver. It is characterized by aggressive growth, early metastases through the cerebrospinal uid seeding the leptomeninges, and invasion of adjacent brain and spinal cord. The common associated nding of hydramnios may be due to impaired fetal swallowing. Hemangioma: Localized proliferation of vascular tissue which rarely presents as fetal neck masses Complex sonographic appearance with many small vascular channels and an almost solid appearance. Progress in molecular and inherited cancer syndromes has led to the further understanding of carcinogenesis. Isaacs H Jr: Tumors of Fetus and Infant: An Atlas, Springer-Verlag, New York, 2002. Microscopically a keratinous plug and an intra or subcorneal vesicle communicates with the underlying sweat duct, sometimes with a mild inammatory inltrate. Milia are pearly yellow 1 to 3-mm papules on the face, chin, and forehead of 50% of newborns. Although milia usually resolve without treatment during the rst month of life, they may persist for several months. Microscopically they are miniature epidermal inclusion cysts, which arise from the pilosebaceous apparatus of vellus hairs. Seborrheic Dermatitis the scalp is most often affected in the newborn and is often associated with in complete removal of the vernix caseosa. The lesions are poorly dened, yellow red salmon-colored patches covered by waxy, greasy, easily removed scales. Section of skin of a newborn showing cyst containing kerati naceous and colloid material. Acanthosis, edema, and occasional perivascular inltration of leukocytes are present as well as spongiosis of the basal layer seen microscopically (Fig ure 21. Leiner disease (desquamative erythroderma) isamoresevereformofse borrheic dermatitis. This condition on the body is erythematous and covered by gray-white brawny or greasy scales. Intermittent fever, diarrhea, generalized lymphadenopathy, edema, and albuminuria may be present. They are char acterized by a separation within the epidermis or between the epidermis and dermis with clefts that may be subcorneal, intraepidermal, suprabasal, A B 21. It begins with skin tenderness, erythema, a scalded appearance, and cleavage of the epidermis and is associated with skin and enteric infec tions. The lesion is an extensive necrosis and inammation of epidermal cells and cleavage of most or the entire epidermis, which produces vesiculobullous lesions. Staphylococcal Scalded Skin Syndrome (Ritter Disease) Thisclinicallyresemblestoxicepidermalnecrolysis. Microscopically there are mild changes in the necrolysis) with desquamation of skin. It presents with variably pruritic vesi clesandbullaeusuallylocatedontheperineum,thighs,buttocks, and lower abdomen, and less commonly on the arms, face, and legs. The vesicles are caused by separation of the basal layer from the basement membrane with neutrophils and eosinophils. It has a characteristic immunouorescence pattern with a linear IgA deposition in the basement membrane. Acrodermatitis Enteropathica this is an autosomal recessive vesiculobullous disease due to a zinc deciency. The lesions are weeping, crusted erythematous patches affecting the diaper region, perioral, acral, and intertriginous areas (Figure 21. It may present in the neonatal period with diarrhea, anooral dermatitis, and alopecia. Affected infants have a defect in zinc binding protein in the gastrointestinal tract with resultant zinc malabsorption. Breast milk is protective because it contains a zinc binding ligand that facilitates zinc absorption. Acquired forms of this disease occur in infants receiving hyperalimentation with a low or absent zinc content and in malabsorption states (cystic brosis, chronic diarrhea, short bowel syndrome). Incontinentia Pigmenti Incontinentia pigmenti is an X-linked dominant trait and is lethal in males. This is followed by verrucous pigmented hyperkeratosis and nally symmetrical hyperpigmentation. Ichthyosis the most severe form of ichthyosis occurs as the harlequin fetus, which is inherited as an autosomal recessive characteristic and is present at birth (Figure 21. The skin is extremely hyperkeratotic with large, rigid plaques between which are ssures imparting a grotesque appearance. The hands may appear moist and weeping with no apparent skin covering, and the nails may be A B 21. This infant developed thick plate-like scales and ectro pion immediately after birth followed by respiratory failure and death. The collodion baby (lamellar ichthyosis) is encased in a thick cellophane-likemembranewithanincidenceof1/300,000births. The skin is rough and scaly, and the lesion is most prominent on the extensor surfaces, especially elbows and knees. X-linked ichthyosis is characterized by generalized large, dark scales with sparing of the palms and soles. In one-third, the lesions are present at birth; the incidence is 1/6,000 male births. Prenatal diagnosis by fetoscopic skin biopsy in all forms of ichthyosis is possible. Menkes kinky hair syndrome is X-linked due to a defect in intestinal copper absorption resulting in a low serum copper level and low ceruloplasmin. An eyebrow hair biopsy by fetoscopy has conrmed the diagnosis in a 20 week fetus (Figure 21. These lesions last 3 or 4 days and usually disappear with no sequelae, but in malnourished or compromised infants secondary infection may cause serious illness. Microscopically the dermis is edematous with intense eosinophilic inltra tion with a few neutrophilic polymorphonuclear and mononuclear cells in a perivascular distribution. Skinbiopsyrevealshyperkeratosis,acanthosis,andintracornealvesicleswith small collections of neutrophils, eosinophils, and keratinous debris. Acropustulosis of Infancy Infantile acropustulosis may be present in the neonatal period. It is charac terized by crops of very pruritic, recurrent vesiculopustules ranging from 1 to 3 mm in diameter. Microscopically, there is focal intraepidermal necrolysis followed by the for mation of vesicles that become lled with neutrophils and eosinophils. Candida Infection Candida colonizes the gastrointestinal tract and skin shortly after birth and may produce both localized (thrush and diaper dermatitis) and disseminated cutaneousinfectionaswellassystemicinfectioninthenewborn(Figure21. This lesion also should raise the suspicion of heritable or acquired immunod eciency. Recurrent and persistent infection in infancy may be associated with the use of antibiotics. Syphilis the skin lesions of congenital syphilis are the result of an intrauterine syphilitic infection (Figure 21. In macerated stillborn fetuses, spirochetes can be detected, andthereishepatosplenomegaly,nucleatedredbloodcellsinvillouscapillaries, and chorioamnionitis. Rhagadesdevelopintherstfewdaysoflifeasmoist,ul cerating lesions extending outward in a liner manner from the angles of the eyes, nose, and mouth. Herpes Simplex this infection results from inoculation from genital herpes inthemother. A skin rash occurs in 70%, and 90% of those infants develop systemic disease with lung, liver, gastroin A testinal, and brain involvement with high mortality. Infantwithascalyeruptionreminiscentofthelesionsofsecondary syphilis may appear on the face, trunk, and extremities. It is a dermatomal cutaneous infection caused by reactivation of varicella-zoster virus in the mother. It is a generalized infection with involvement predominantly of the brain, liver, and spleen as well as the skin. It consists of sharply dened, nonelevated areas of subcutaneous induration B that appear a few days after birth in large, well-developed, otherwise healthy 21. The lesions are woody in consistency and do not pit on pressure; traepidermal vesicle (bottom). Sclerema Neonatorum this lesion appears to be a complication of multisystem fail ure with cooling of the skin and subcutaneous adipose tissue from decreased cutaneous perfusion. It is characterized by a widespread induration of the skin that begins between the third and fourth day after birth. It appears rst on the legs or face and in a short time may involve all the body surfaces except the palms, soles, and scrotum. The affected areas are smooth, hard, dry, cold to touch, and whitish or waxy in appearance. The condition is limited almost exclusively ant cells and refractile crystals representing triglycerides are to premature infants. Absent nipples, elbow and hip con tractions, skin thicker across buttocks, patulous everted anus, no gluteal crease. The sagittal suture is 6 cm across, brain shows through dura, cataracts, membrane across nares, mouth, and ears. Scleredema usually appears as a diffuse waxlike hardening of the skin in a severely ill newborn from the second to the fourth day after delivery. Intense edema with mild nonspecic changes such as dilation of the vessels, edema, and minimal inammation in the skin, the subcutaneous tissue, and sometimes the underlying muscle characterize the lesion. Theepidermisishyperplastic,keratinproteinsarequantitatively abnormal, and, ultrastructurally, keratin laments are decient and kerato hyalin is abnormal. The skin appendages appear malformed and irregular and the sebaceous glands are increased in number. There is a predis position to basal cell carcinoma and adnexal tumors arising from the lesion, and therefore removal is indicated. Linear Sebaceous Nevus Syndrome this lesion is associated with visceral malformations, including meningeal hemangiomas, congenital heart disease, urinary tract anomalies, nephrob lastomatosis, hydrocephalus, vitamin D-resistant rickets, colobomas, ocular desmoids, seizures, and mental retardation. Congenital Cutaneous Dystrophy (Rothmund-Thomson Syndrome, Poikiloderma Congenitale) this autosomal recessive disease is characterized by skin lesions and congenital cataracts. The skin lesions that are light sensitive early in life begin as a network of ne red lines separating areas of normal skin over part or all of the body.
Your partner can stay with the baby during the brief time that the baby is out of the operating room anxiety helpline purchase luvox online now. After the procedure anxiety treatment without medication luvox 100mg line, you will be in the recovery room with your family until your anesthesia wears off anxiety symptoms ruining my life cheap 100mg luvox fast delivery. The baby remains with you during the entire hospitalization unless you request the nurses to watch the baby in the nursery anxiety issues buy luvox us. The nurses will ask you to stand during the first day and then start walking soon after anxiety symptoms stuttering cheap luvox 100mg online. Ibuprofen is also given to increase the effectiveness of the narcotic (Tylenol with Codeine anxiety symptoms breathlessness order luvox 50mg, Vicodin or Percocet) and decrease the discomfort from uterine contractions after delivery. Labor Induction Labor can be initiated by your physician for medical reasons or electively. Induction can be initiated with a cervical ripening agent (misoprostol or cervidil), by breaking the amniotic sac or with pitocin. If your doctor recommends induction, the indication and the process will be discussed in detail. Call Labor and Delivery at least 2 hours before your scheduled induction time to see if you can go in as scheduled. If the hospital is busy due to already laboring patients, the labor and delivery nurses will ask you to arrive at a later time, and if your induction is semi-elective, there is a chance that you will have to be rescheduled to another day. Reasons for induction include postdates (usually one week past your due date), a history of complications in labor, premature rupture of membrane (water breaking early), high risk pregnancy (diabetes or hypertension), low amniotic fluid, macrosomia (big baby) or elective (after 39 weeks). If you have had a vaginal delivery, schedule an appointment 6 weeks after delivery, unless otherwise instructed by physician. Walking is better for you than running or lifting weights the first six weeks after birth. You probably should not carry anything heavier than the baby for the first week or two. Do not use a Jacuzzi until the vaginal discharge stops or bathe after a cesarean section until the incision is healed (usually 5-7 days). Intercourse is permissible after the vaginal discharge and bleeding stop, usually at three to four weeks. Condoms should be used with a water-soluble lubricant such as K-Y jelly or Astroglide. Vaginal Delivery After delivery, you will experience bleeding and a discharge for 4 to 6 weeks. If you had a vaginal tear or episiotomy, your vaginal area may be swollen or sore. Taking sitz baths or a warm bath 2 to 3 times a day will help with the discomfort and promote healing. Cesarean Section Cesarean section incisions have many layers that heal at the same time. Call the office for an appointment if your incision opens, has a large amount of discharge or bleeding, or if it becomes red or painful. If you are breast-feeding and took prenatal vitamins during your pregnancy, continue them while nursing. Fiber supplements and stool softeners (Colace) are available without a prescription. If you become constipated with no bowel movement for a few days, you may need a laxative such as Miralax, Ducolax or Senakot. Medications You may also continue to use the same medications used during your pregnancy. Anti-inflammatory Medication Ibuprofen and Naprosyn are nonprescription pain relievers that reduce cramping, bleeding and discomfort. The usual dose of Ibuprofen (Advil, Nuprin, Motrin) is 600 mg every 6 hours, not to exceed 2400 mg in 24 hours and Naprosyn (Aleve) is 220 mg, 2 initially, then 1 every 6-8 hours, not to exceed 1100 mg in 24 hours. Tylenol is also useful for pain relief and can be taken with Ibuprofen and Naprosyn as they work differently. Narcotics Percocet, Vicodin, or Tylenol #3 are narcotics that may be prescribed by your physician if you have had a cesarean section. Ibuprofen and Naprosyn work synergistically with the narcotic so that you need less of it. Continue the anti-inflammatory medication after you stop taking the narcotic to continue with pain relief. The second is watery-pink, lasting for 1-3 weeks, and the third is yellowish-white, lasting another 3-6 weeks. Clots can be bright red, dark red, small or large and are frequently associated with severe cramping. Call for excessive bleeding, soaking one pad per hour with bright red blood or continuing to pass large clots. The edges of the incision may be more swollen than the center because of knots used to close the layers located at the sides of the incision. The top of the incision frequently hangs over the lower edge during the healing process until the lymphatic system begins to function normally. Call the office if the incision becomes red, more inflamed, more tender, or begins to leak fluid. Constipation Hormonal changes, dehydration, breast-feeding and inactivity cause constipation. Try increasing the fiber in your diet, drinking more water, and using stool softeners. We recommend changing your position often, emptying your bladder often, using a heating pad, and taking Ibuprofen to help with the contractions. Depression and Emotional Changes It is normal to feel overwhelmed, exhausted, and sleep deprived. The lifestyle changes, exhaustion, and fluctuating hormones frequently cause anxiety and feelings of helplessness. The demands of a new baby and inadequate sleep may lead to feelings of depression. Resting, maintaining a good diet, and planning time for you away from baby are important. If depression persists longer, or seems more severe, please do not hesitate to schedule an appointment with your doctor. Engorged Breasts Try using ice packs and wearing a sports bra or nursing bra all the time. If you are nursing, your body should regulate the engorgement within the first few weeks. Episiotomy 69 Use ice packs the first 1-2 days and Ibuprofen as needed for swelling and discomfort. Taking a warm bath, using a sitz bath, a spray bottle, or a rubber ring/donut to sit on may also help. Hair Loss Thinning hair is normal postpartum, with the most noticeable change 5-6 months after delivery. Hormonal Changes It is common after delivery to experience hot flashes, night sweats, mood swings, and vaginal dryness similar to what women experience in early menopause. Your estrogen level drops with delivery and is reduced until you finish nursing and your regular menses resumes. If the symptoms are troublesome, you can discuss estrogen replacement with your physician. A small dose of oral or transdermal (patch) estrogen will reduce the vasomotor symptoms of hot flashes and night sweats. The body treats nursing like menopause with all the same symptoms due to lack of estrogen. Starting a combination oral contraceptive pill or using an estrogen patch usually helps decrease the symptoms. Sex If you had a cesarean section or a vaginal delivery without an episiotomy, you may attempt intercourse four weeks after delivery. If you had a vaginal delivery with an episiotomy or laceration, wait until after your postpartum visit. You may need to use lubrication (Astroglide or K-Y Jelly), especially if you are breastfeeding. If vaginal dryness persists, vaginal estrogen cream can be prescribed by your physician. Urinary Leakage Urinary stress incontinence is caused by decreased perineal muscle tone and lack of estrogen. Using estrogen vaginally (prescription) can also help restore the tissue if dryness is an issue. Breast feeding on demand will help reduce engorgement and increase the milk supply. Try to nurse your baby for at least 15 minutes on one breast and for about 10 minutes on the other breast. Breast milk can be stored in a sterile container in the refrigerator for up to 72 hours or in a standard freezer for 1-2 weeks. Mastitis (breast infection) You may be developing mastitis if you have a high fever associated with a painful, red breast. Other signs of a breast infection include increased pulse rate, chills, malaise, headaches, and an area on the breast that is red, tender, and hard. Treatment involves antibiotics, rest, frequent breastfeeding or pumping, and analgesics for pain and fever. There is no medication approved by the Food and Drug Administration to prevent engorgement. LactMed is a database of medications that women might be exposed to while breastfeeding. It contains information about the medication, ways it might affect the mother or baby, and potential alternatives to consider. Rhythm Intercourse is timed to avoid the fertile period during a menstrual cycle, using body temperatures and graphs, and avoiding intercourse during these fertile times. Vaginal Spermicide Foams, suppositories, tablets, or jellies are inserted into the vagina before intercourse. Diaphragm A vaginal barrier method used in combination with spermicidal cream or jelly. Nexplanon A small, thin, implantable progesterone contraceptive that is effective for up to three years and is placed under the skin in the forearm. It is used frequently while nursing because it does not decrease the quantity of breast milk. It suppresses ovulation, diminishes growth of the endometrium, and increases the thickness of mucus around the cervix, preventing the passage of sperm through the cervix. Depo Provera (Contraceptive Injection) 74 A progesterone injection that stops ovulation and prevents sperm from entering the uterus. It is given every 12 weeks (3 months) and starts working within 24 hours after injection. Nuvaring and OrthoEvra A vaginal ring or patch that secretes both estrogen and progesterone locally into the uterus and vagina to prevent ovulation and implantation. An incision is made over the vas deferens on each side of the scrotum to cut the ducts and prevent active sperm from release. The procedure is usually performed by a Urologist in his office under local anesthesia. Tubal Sterilization (Female) this is a surgical procedure to permanently cut or remove the fallopian tubes. This procedure can be performed at the time of cesarean section, the time of delivery or later as an outpatient surgery. Usually there are at least four noticeable movements or "kicks" most hours of the day. When you are busy during the day, you may not notice your baby moving as much as when you are at rest. Kick counts should be done with an empty bladder about one hour after a meal, while resting on your left side to promote circulation. To perform kick counts, pay attention to any kick or rolling movement of the baby. If by one hour you have not been aware of four movements, you may have been too busy with other activities. If you still have not noted four movements in the next hour, telephone the office (even on weekends and holidays). You may be requested to come into the office or to go to the hospital for further evaluation. A small number of cells are taken from the placenta and are diagnostic for Down syndrome and Trisomy 18.
Buy genuine luvox on line. ANXIETY DISORDER Symptoms and Treatments.