Bang Huynh, MD
- Chief, Thoracic Imaging
- David Grant USAF Medical Center
- Travis AFB, California
Close contacts are considered to be individuals who have slept in the same house as the patient at any time in the 7 days before onset of symptoms erectile dysfunction treatment lloyds buy erectafil 20 mg mastercard, and boyfriends or girlfriends of the patient top erectile dysfunction doctor cheap erectafil 20 mg fast delivery. Only healthcare workers who have administered mouth-to-mouth resuscitation or had prolonged face-to-face con tact with the patient require prophylaxis and this should be initiated after consultation with the hospital infection control team muse erectile dysfunction wiki cheap erectafil 20 mg on-line. Prophylaxis for other contacts from closed communities such as nurseries erectile dysfunction getting pregnant generic erectafil 20mg on line, schools or universities should be considered where two or more linked cases have occurred and this should be initiated by a public health doctor erectile dysfunction natural cure order cheap erectafil on-line. Smoking is a risk factor for carriage of the meningococcal bacteria and the patient should be referred to a stop smoking service erectile dysfunction doctor boca raton cheap erectafil online amex. Neuropathy of the sensory, motor and autonomic nerves, along with micro vascular and macrovascular disease and impaired neutrophil function all contribute to the development of foot ulcers in diabetic patients. Features associated with infection include cellulitis, lymphangitis, puru lent drainage, sinus tract formation, osteomyelitis, septic arthritis, abscess 130 Pharmacy Case Studies formation and sometimes the development of gangrene. Systemic manifesta tions may include fever, tachycardia, confusion and hypotension. Neuropathy and ischaemia may obscure or mimic these cardinal signs of in am mation in patients with diabetes and experts have suggested that antibiotics are indicated in patients with evidence of cellulitis, fever, leucocytosis, foul smelling wounds or deep tissue infection (Cavanagh et al. Diabetic foot ulcers are often colonised by multiple organisms that may or may not be pathogenic, therefore a swab of the ulcer surface is unreliable for iden tifying causative organisms in infection. The most reliable sample for culture is a specimen of deep tissue obtained by aspiration or biopsy without contact with the ulcer surface or draining lesions. Mild ulcers are frequently infected by Staphylococcus aureus and Streptococcus pyogenes (group A strep). Other pathogens include Gram-negative rods and anaerobic bacteria (although anaerobes are seldom successfully cul tured). Gram-positive pathogens include Staphylococcus aureus, Staphylococcus epidermidis (coagulase negative staphylococcus), streptococci, enterococci, corynebacteria (diph theroids) and clostridia. Gram-negative pathogens include Enterobacteriaceae (coliforms) such as Escherichia coli, Klebsiella, Proteus and Pseudomonas species. The need to be right this is an important principle which governs selection of empirical therapy. If a patient has a severe or life-threatening infection or if they are vulnerable (for example due to immunocompromise), the empirical therapy regimen must be broad spectrum enough to encompass the majority of likely pathogens. Bearing in mind that broad-spectrum anti-infectives are not necessarily the most effect ive agents against speci c pathogens, the regimen can later be streamlined to narrower spectrum agents once the pathogen(s) and anti-infective sensitivities are known. Previous microbiology results may in uence the choice of empirical treatment providing they are within a reasonable timeframe and representative of infection rather than colonisation. Infections case studies 131 the risk of resistant organisms Whether an infection is community-acquired or healthcare-acquired is of fundamental importance in choosing empirical therapy. Community-acquired infections tend to be caused by pathogens that are typically sensitive to a wide range of rst-line anti-infectives. Healthcare-acquired infections in contrast are often caused by multi-resistant pathogens by virtue of the characteristics of the healthcare environment, including intensive anti-infective use and close cohorting of vulnerable patients. Patients who have failed an anti-infective regi men at adequate dosing are also more likely to have resistant organisms. Contraindications and cautions the major groups of patients to whom contraindications may apply are patients with a history of hypersensitivity, pregnant or breastfeeding women, patients with organ dysfunction and the very old and very young. The regimen should ideally cover the organisms identi ed from his previous microbiology specimens, although these may be unreliable if taken from the surface of the ulcer. Intravenous administration affords greater pene tration of the anti-infective to areas of poor perfusion. The patient is on gabapentin but this is for neuropathic pain rather than epilepsy so uoroquinolones may be used. Alternatives to piperacillin-tazobactam for a penicillin-allergic patient with infected diabetic foot ulcer include: I Clindamycin (to cover staphylococci, streptococci and anaerobes) plus gentamicin, cipro oxacin, ceftazidime or aztreonam (to cover Gram-negative organisms including Pseudomonas). Serum creatinine indicates mild renal impairment which may in uence choice and monitoring of antibiotic therapy. Leucocytosis is an indication of infection but this may be absent in patients with diabetes. If osteomyelitis is ruled out, then shorter courses of antibiotic therapy are likely to be required for successful clinical outcome. Debridement and drainage are critical aspects of management of the infected diabetic foot ulcer and delayed debridement of necrotic or infected tissue and drainage of purulent collections increases the risk of amputation. Wound man agement is also extremely important and use of vacuum foam dressing may be required to remove exudate and slough and promote granulation. Medicated dressings such as hydro bre dressings impregnated with silver provide a local antiseptic effect where poor blood supply may limit antibiotic penetration. An evidence-based guideline for diabetic foot infections from the Infectious Diseases Society of America highlights the lack of published clinical trials of antibiotics for this indication. The use of differing de nitions of infec tion severity and clinical outcome makes comparison of antibiotic ef cacy between studies unreliable. The guideline concludes that on the basis of avail able studies, no single drug or combination of agents appears to be superior to others (Lipsky et al. The identi cation of Gram-positive cocci in blood cultures in this case mandates use of reliable Gram-positive cover such as vancomycin or teicoplanin or one of the newer agents: linezolid, daptomycin or tigecycline. These agents Infections case studies 133 are all suitable for patients with penicillin allergy. The patient has mild renal impairment but vancomycin may still be used providing appropriate dose adjustments are made and therapeutic drug monitoring is carried out. The severity of infection suggests that Gram-negative cover would also be prudent. Gentamicin is associated with increased nephrotoxicity in combina tion with vancomycin and cipro oxacin offers an alternative option providing the patient is not at signi cant risk of seizures. A malodorous wound is consistent with an anaerobic infection requiring suitable anaerobe cover such as metronidazole or clindamycin. Oral agents may be selected from rifampicin, tetracyclines, fusidic acid or trimethoprim depending on sensitivity data and a combination of two agents is recommended. The goals of therapy are to rapidly control the infection and stabilise the patient to minimise morbidity and mortality and reduce the risk of amputation. Resolution of local and systemic symptoms and signs of infection are the primary indicators of improvement. Foot ulcers cause signi cant morbidity and impaired quality of life and are the most important risk factor for lower extremity amputation. Pharmacists can play an important role in patient education around self-care and self-monitoring of the feet. Patients should be advised to check their feet daily for problems and to wash in warm (not hot) water and carefully dry their feet daily. They should be encouraged to wear well tted shoes and hosiery and cautioned against skin removal, including corn removal, without expert help. Over-the-counter pre parations for foot problems such as corn removal are not suitable for patients with diabetes. Good control of blood glucose is paramount in preventing complications of diabetes mellitus including diabetic foot ulcers. Pharmacists should support concordance with oral hypoglycaemic and insulin regimens and regular blood glucose monitoring. Scenario Mr Jones, a regular customer in your shop, hands you over a prescription. He recently took early retirement from his job as an Of ce Clerk as he was getting extreme fatigue in all his muscles, especially after a long day at work. He had spoken to you a few months ago about the fatigue and thought that it may be due to stress or poor diet, as he had been working very long hours to complete a contract on time. He bought some multivitamins with ginseng, but his tiredness did not improve except when he had a few days holiday. National Institute of Neurological Disorders and Stroke (2008) Myasthenia gravis fact sheet. Scenario Mrs Smith, who is 35-years-old, comes into your pharmacy with her 1-year-old daughter and gives you a prescription for levothyroxine 50-microgram tablets take one daily. She has gained a lot Endocrine case studies 137 of weight since the birth of her daughter and has not been able to shift it even by sticking to a calorie-controlled diet. She has no energy at all, whereas before the birth of her daughter she used to go to aerobics at least three times a week. Questions 1 What condition does Sally have and what are the usual signs and symptoms She wants your opin ion as the orthopaedic consultant has said she has got osteoporosis and wants to send her for a special X-ray and start treatment. Comment on their advantages and disadvantages with regards to Mrs Patel, using the latest evidence. Endocrine case studies 141 Scenario You are a supplementary prescriber working in a diabetes clinic when John Stephens comes in to see you. He is still overweight despite being on the maxi mum dose of metformin and gliclazide. General references Clinical Knowledge Summaries (2002) Type 2 diabetes-blood glucose. In myasthenia gravis antibodies block, alter or destroy the receptors for acetylcholine at the neuromuscular junction, which prevents the muscle contraction from occurring. Hence with fewer receptor sites available the muscles receive fewer nerve signals. The patient has muscle weakness which increases after a period of activity and improves with rest. He has drooping of the eyelids (ptosis) with blurred vision due to weakness of the muscles that control eye movement. Myasthenia gravis most commonly affects young adult women (under 40) and older men (over 60) and is not inherited. Risk factors include fatigue, illness, stress, extreme heat and other medication (including beta-blockers, calcium channel blockers, quinine and quinolones). An intravenous injection of edrophonium chloride which is a drug that blocks the degradation of acetylcholine and temporarily increases the levels of acetylcholine at the neuromuscular junction. It should demonstrate decrements of the muscle action potential due to impaired nerve-to-muscle transmission. It is less powerful and slower in action than neostigmine but it has a longer dura tion of action. It has relatively mild gastrointestinal effect but an antimuscarinic drug may still be required for the stomach cramps. A total daily dose of 450 mg should not be exceeded in order to avoid acetylcholine receptor downregulation. Immunosupressant therapy is usually added if the dose of pyridostigmine exceeds 360 mg daily. It is only available as a tablet, unlike neostigmine which comes as a tablet and injection. What should the normal range be for the laboratory test results and what levels would you expect Mrs Smith to have before treatment Oral contraceptives and hormone replacement ther apy can falsely raise total T4 levels, so free T4 should be measured if Mrs Smith takes these drugs.
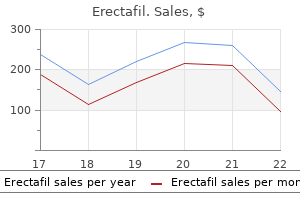
The graph obtained is one of absorbance (dependent on protein concentration) vs time erectile dysfunction blood pressure medication buy genuine erectafil online. It consists of 5 zones erectile dysfunction vascular causes order erectafil toronto, namely from anodally: albumin erectile dysfunction xanax order generic erectafil, alpha 1 erectile dysfunction medication class discount erectafil 20mg on-line, alpha 2 injections for erectile dysfunction that truly work buy generic erectafil 20mg on line, beta and gamma zocor impotence order 20 mg erectafil mastercard. Transthyretin complexes with retinol binding protein, preventing filtration by glomeruli. Prealbumin decreased in hepatic damage, acute phase inflammatory response and tissue necrosis. Elevated levels are seen in patients on steroids, in alcoholism and chronic renal failure. Surgery, trauma, myocardial infarction, baterial infections and tumours are conditions eliciting an inflammatory response. Uninhibited elastase action leads to emphysema Increased levels occur during the acute phase response (synthesis stimulated by cytokines) and with increased estrogen (increased synthesis). Smoking aggravates the problem by recruitment and activation of leukocytes, and by generating free radicals. These oxidize a methionine at the 1 antitrypsin active site, and thereby inactivate it. Deficiency should be suspected when the 1 band is decreased on electrophoresis, 1 antitrypsin being the main constituent of the 1 region. Confirmation of 1 antitrypsin deficiency requires accurate measurement of serum levels using specific immunological techniques. Analytical methodology: major constituent of the 1 globulin region on serum protein electrophoresis. The haptoglobin-haemoglobin complex is removed rapidly by the reticulo-endothelial system, this prevents loss of haemoglobin in urine, & conserves iron. Elevated levels are associated with acute phase response, nephrotic syndrome and with corticosteroids. Analytical methodology: migrates to 2 region on serum protein electrophoresis; immunoturbidimetry. Acts like a primitive antibody, and when complexed activates the complement cascade. Protease inhibitor binds to all proteases and inhibits by enfolding them and preventing substrate access. The protease 2 macroglobulin complex is rapidly cleared by the reticulo-endothelial system. Causes a marked increase in the alpha 2 region of the plasma electrophoretic profile in nephrotic syndrome, since low albumin induces a generalized increase in hepatic protein synthesis the small proteins are lost in the urine but large (2 macro and lipoprotein i. It is freely filtered and is normally reabsorbed and degraded in the proximal convoluted tubule. Urine levels increase in renal tubular damage and one of its main uses is in monitoring of nephrotoxic drugs. Cerebrospinal fluid contains an enzyme (neuraminidase) which cleaves off neuraminic acid residues from some of the transferrin, altering the charge (becomes less negative) and hence causing transferrin to migrate to the 2 region on electrophoresis. Secondary far more common than primary accompanied by increased risk of infection. IgM reaches adult levels by 9 months of age, IgG has adult levels at birth (from maternal IgG crossing the placenta in the last trimester of pregnancy), reaches a nadir (lowest point) by 3 months of age, and reaches adult levels by about 3 years of age. It is caused by the proliferation of a single clone of B cells producing an Ig containing a single light chain and heavy chain type only. Occasionally the peak may not contain complete Ig molecules but only light or only heavy chains, if the aberrant clone produces either predominantly. IgG (50%), IgA (20%), light chains (15%) are the more common while IgD (2%), IgE (<1%) and IgM myelomas are rare. Can only be called benign after being shown to be stable for 5 years (IgG & IgA) and for 10 years (IgM). These patients have circulating M-protein levels of less than the 30g/L required for a diagnosis of myeloma, with a bone marrow plasma cell count of less than 10%. The risk of progression in 10years is approximately numerically equal to the M-protein in g/L. Clinical evaluation and paraprotein levels should be reviewed at 3 and 6 months to establish diagnosis. Type I: this type is monoclonal in nature, with absent Rheumatoid Factor activity. These monoclonals do not activate complement effectively and thus do not usually present with vasculitis, rather hyperviscosity. Precipitation at lower temperatures seldom occur in vivo and hence never produce symptoms. These proteins are arranged in sheets (consisting of rigid, non-branching fibrils arranged in zigzags) which can be identified by apple green fluorescence on Congo red staining. Beta sheets are thought to form when proteins misfold (due to structural instability) and then self-aggregate, forming fibrils. Specific amyloidoses involve specific organs (specific proteins target defined organs). Patients most commonly present with renal disease, but may also present with hepatomegaly and/or splenomegaly. In patients with a family history, isoelectric focusing will separate wild-type transthyretin from variants, after which genetic testing can be done to determine the mutuation. Damage to foot processes in minimal change nephritis selective proteinuria (steroid responsive) b. More severe damage to glomeruli gives a non-selective proteinuria not steroid responsive Selectivity assessed by: i. Haem pigments: all have peroxidase activity which results in oxidation of o-toluidine (available on test strips) a. True haemoglobinuria occurs when severe intravascular haemolysis exceeds haptoglobin binding capacity. Myoglobinuria from muscle injury: As for haemoglobinuria but myoglobin can be differentiated from haemoglobin on size basis using gel filtration chromatography. Approximately 10-12 ml can be taken from an adult and less than 3 ml from a neonate. The tubes should be labelled with a number indicating the order in which they were collected. At the same time blood should be drawn simultaneously for serum glucose measurement as well. Apart from direct organism identification, biochemistry and cell counts can help distinguish between the types of meningitis. All xanthochromic fluids will have elevated lactate levels, so it is best not to measure lactate in these fluids. Cisternal and ventricular fluids have lower total protein concentration than fluid obtained by lumbar puncture. A test referred to as the net bilirubin absorbance, is sometimes requested by neurosurgeons. The determination of net bilirubin absorbance is performed by scanning the sample at different wavelengths to determine if there is bilirubin present or whether there is haemoglobin. These can be distinguished by the wavelengths at which they show maximal absorbance. The preferred term is Asialotransferrin) in the fluid leak sample, using electrophoresis and immunofixation. Bamyloid, a sticky protein fragment abnormally cleaved from a larger precursor protein called amyloid precursor protein, concentrations are significantly lower in csf samples. Other markers that may be raised include angiotensinconverting enzyme; lysozyme and 2-microglobulin. These further subdivide to provide hepatic arterioles and portal venules which run in portal tracts together with bile canaliculi, lymphatics and nerves. Three to four portal tracts lie perpendicularly in the septae at the periphery of each hepatic lobule. It is centrally divided by the connective tissue septum in which runs a small branch of the portal tract containing terminal branches of the hepatic arteriole and portal venule. The parenchymal liver cells (hepatocytes) are arranged in columns (plates) extending from the septum to the centrilobular venule, with vascular spaces (sinusoids) between them. The sinusoids are separated from the hepatocytes by the space of Disse 223 Blood flows from the portal tract, through the sinusoids, and drains into the centrilobular venule. Hepatocytes also metabolise and detoxify endogenous (haem) and exogenous products (drugs), which are then excreted via the biliary tree. Haem (a 4 ring structure containing Fe at its centre) is broken down (via biliverdin) to carbon monoxide, iron and bilirubin. This canalicular excretion step rather than conjugation is thought to be the rate-limiting step in bilirubin metabolism. In the absence of bowel flora (newborns, broad spectrum antibiotic therapy) faeces are yellow due to bilirubin. The rate limiting and regulated step in their formation is 7 hydroxylation of cholesterol. Re-uptake of bile acids by the liver is highly efficient, but sensitive to liver damage. This facilitates the formation of micelles when mixed with triglyceride or other lipids, and allows lipid absorption. Normal urine contains no bilirubin, since unconjugated bilirubin is albumin-bound and not filtered. This explains why conjugated hyperbilirubinaemia may occasionally persist even after bilirubinuria has disappeared). The usefulness of serum enzymes as markers of liver disease is limited by the fact that they are also found in and released from other tissues. It is therefore more useful to look at all the parameters of liver function (or at least all of the enzymes) rather than at one single enzyme. It is an ecto-enzyme, located on the outside of the cell membrane (canalicular side of liver cell). It is involved in the transport of amino acids across the liver cell plasma membrane. Serum level increased by cholestasis or chronic ingestion of alcohol, barbiturates, phenytoin and other drugs which induce the enzyme. It is increased markedly in primary liver cell carcinoma (hepatoma) as a result of reversion of the malignant cells to a de-differentiated state. Moderate elevations may occur when liver tissue is regenerating, such as in the recovery stage after hepatitis or in cirrhosis. Measurement of ammonia is most useful in cases of altered levels of consciousness, since elevated ammonia levels are responsible for the neurological signs of hepatic encephalopathy. Diagnosis is made on the basis of hyperammonaemia and specific amino acid abnormalities in plasma and urine (see Inborn Errors of Metabolism lectures). The liver has a large reserve capacity jaundice only appears with severe impairment of liver function. Later marked increases as intrahepatic cholestasis develops due to swelling of cells. Transaminases only elevated if cholestasis is severe enough to cause secondary hepatocellular damage. Irrespective of aetiology, the classification, prognosis and treatment are based on the histological features.
Buy erectafil overnight delivery. Tom and Jerry 36 Episode - Old Rockin' Chair Tom (1948).
But it may not be suitable for larger tumors or those that are close to the surface of the skin erectile dysfunction jason purchase erectafil without prescription. The risk of local cancer recurrence with this type of mastectomy is the same as with other types of mastectomies erectile dysfunction medicine in homeopathy purchase generic erectafil pills. Nipple-sparing mastectomy Nipple-sparing mastectomy is a variation of the skin-sparing mastectomy erectile dysfunction low testosterone treatment purchase 20mg erectafil amex. The surgeon often removes the breast tissue beneath the nipple (and areola) during the procedure to check for cancer cells erectile dysfunction treatment jaipur purchase erectafil canada. Afterward injections for erectile dysfunction order erectafil with a mastercard, the nipple may not have a good blood supply erectile dysfunction treatment without medicine buy erectafil 20 mg without a prescription, causing the tissue to shrink or become deformed. Because the nerves are also cut, there often may be little or no feeling left in the nipple. If a woman has larger breasts, the nipple may look out of place after the breast is reconstructed. As a result, many doctors feel that this surgery is best done in women with small to medium sized breasts. This procedure leaves fewer visible scars, but it also has a risk of leaving behind more breast tissue than other forms of mastectomy. This could result in a higher risk of cancer developing than for a skin-sparing or simple mastectomy. Improvements in technique have helped lower this risk and experts consider nipple-sparing mastectomy to be an acceptable treatment for breast cancer in properly selected women. Modified radical mastectomy A modified radical mastectomy combines a simple mastectomy with the removal of the lymph nodes under the arm (called an axillary lymph node dissection). The surgeon removes the entire breast, axillary (underarm) lymph nodes, and the pectoral(chest wall) muscles under the breast. This surgery was once very common, but less extensive surgery (such as the modified radical mastectomy) has been found to be just as effective and with fewer side effects. This operation may still be done for large tumors that are growing into the pectoral muscles. Double mastectomy When both breasts are removed, it is called a double (or bilateral) mastectomy. Most of these mastectomies are simple mastectomies, but some may be nipple-sparing. This is done after careful consideration and discussion between the patient and their cancer care team. You may have an initial gut preference for mastectomy as a way to "take out all the cancer as quickly as possible. It does not lower the chance of the cancer coming back in other parts of the body, including the opposite breast. Breast reconstruction surgery after mastectomy After having a mastectomy a woman might want to consider having the breast mound 19 American Cancer Society cancer. Although each case is different, most mastectomy patients can have reconstruction. Insurance companies typically cover breast reconstruction, but you should check with your insurance company so you know what is covered. Wearing a breast prosthesis (breast form) is an option for women who want to have the contour of a breast under their clothes without having surgery. Recovering from a mastectomy: What to expect In general, women having a mastectomy stay in the hospital for 1 or 2 nights and then go home. How long it takes to recover from surgery depends on what procedures were done, and some women may need help at home. Most women should be fairly functional after going home and can often return to their regular activities within about 4 weeks. Recovery time is longer if breast reconstruction was done as well, and it can take months to return to full activity after some procedures. Usually, you and your caregivers will get written instructions about care after surgery. These instructions typically cover: q How to care for the surgery site and dressing q How to care for your drain, if you have one (this is a plastic or rubber tube coming out of the surgery site attached to a soft rubber ball that collects the fluid that occurs during healing) q How to recognize signs of infection q Bathing and showering after surgery q When to call the doctor or nurse q When to start using your arm again and how to do arm exercises to prevent stiffness q When you can start wearing a bra again q When to begin using a prosthesis and what type to use q Use of medicines, including pain medicines and possibly antibiotics 20 American Cancer Society cancer. Through our Reach To Recovery 5 program, a specially trained volunteer who has had breast cancer and can provide information, comfort, and support. Side effects of mastectomy the side effects of mastectomy can depend on the type of mastectomy you have (more extensive surgeries tend to have more side effects). As with all operations, bleeding and infection at the surgery site are also possible. Treatment after mastectomy Some women might get other treatments after a mastectomy, such as hormone therapyto help lower the risk of the cancer coming back. If so, radiation therapy and/or hormone therapy is usually delayed until the chemotherapy is completed. Local breast cancer recurrence after mastectomy and immediate breast reconstruction for invasive cancer: a meta-analysis. Last Medical Review: September 18, 2019 Last Revised: September 18, 2019 Lymph Node Surgery for Breast Cancer 1 If breast cancer spreads, it typically goes first to nearby lymph nodes under the arm. It can also sometimes spread to lymph nodes near the collarbone or near the breast bone. Knowing if the cancer has spread to your lymph nodes helps doctors find the best way to treat your cancer. To help find out if the cancer has spread outside the breast, one or more of the lymph nodes under the arm (axillary lymph nodes) are removed and checked in the lab. If the lymph nodes contain cancer cells, there is a higher chance that cancer cells have also spread to other parts of the body. Lymph node removal can be done in different ways, depending on whether any lymph nodes are enlarged, how big the breast tumor is, and other factors. If cancer is found in the lymph node, more nodes will need to be removed during an 23 American Cancer Society cancer. Types of lymph node surgery Even if the nearby lymph nodes are not enlarged, they will still need to be checked for cancer. Lymph node surgery is often done as part of the main surgery to remove the breast cancer, but in some cases it might be done as a separate operation. To do this, the surgeon injects a radioactive substance and/or a blue dye into the tumor, the area around it, or the area around the nipple. Lymphatic vessels will carry these substances along the same path that the cancer would likely take. The first lymph node(s) the dye or radioactive substance travels to will be the sentinel node(s). The surgeon cuts the skin over the area and removes the node(s) containing the dye or radioactivity. The few removed lymph nodes are then checked closely for cancer cells by a pathologist. If no cancer cells are seen in the node(s) at the time of the surgery, or if they are not checked by a pathologist at the time of the surgery, they will be examined more closely over the next several days. Studies have shown however that in some cases it may be safe to leave the rest of the lymph nodes behind. This is based on certain factors, such as the size of the breast tumor, what type of surgery is used to remove the tumor, and what treatment is planned after surgery. If you are offered this type of biopsy, ask your surgeon if they do them regularly. Lymphedema A possible long-term effect of lymph node surgery is swelling in the arm or chest called 6 lymphedema. Because any excess fluid in the arms normally travels back into the bloodstream through the lymphatic system, removing the lymph nodes sometimes blocks drainage from the arm, causing this fluid to build up. It may be more common if radiation is given after surgery or in women who are obese. If your arm is swollen, tight, or painful after lymph node surgery, be sure to tell someone on your cancer care team right away. Limited arm and shoulder movement You might also have limited movement in your arm and shoulder after surgery. Your doctor may advise exercises to help keep you from having permanent problems (a frozen shoulder). Some women notice a rope-like structure that begins under the arm and can extend down toward the elbow. This is sometimes called axillary web syndrome or lymphatic 28 American Cancer Society cancer. This often goes away without treatment, although some women may find physical therapy helpful. Numbness Numbness of the skin on the upper, inner arm is a common side effect because the nerve that controls sensation here travels through the lymph node area. Chapter 79: Malignant 29 American Cancer Society cancer. Axillary dissection vs no axillary dissection in women with invasive breast cancer and sentinel node metastasis. Lymphedema: A primer on the identification and management of a chronic condition in oncologic treatment. Last Medical Review: September 18, 2019 Last Revised: September 18, 2019 30 American Cancer Society cancer. Women with breast cancer often have treatment with some kind of surgery which can include: q Surgical breast biopsy q Lymph node removal q Breast conservation surgery (lumpectomy) q Mastectomy q Breast reconstruction Any of these can affect how well you can move your shoulder and arm or go about your daily activities, like dressing, bathing, and combing your hair. Pain and stiffness can cause weakness and limit movement of your arm and shoulder. Exercises help decrease side effects of your surgery and help you get back to your usual activities. Your doctor might suggest you see a physical therapist or occupational therapist, or a cancer exercise specialist certified by the American College of Sports Medicine. These health professionals are specially trained to design an exercise program just for you. You might need this kind of help if you do not have full use of your arm within 3 to 4 weeks of surgery. Some exercises should not be done until drains and sutures (stitches) are removed. The exercises that increase your 31 American Cancer Society cancer. Talk to your doctor or therapist about which of these are right for you and when you should start doing them. The week after surgery the tips and exercises listed below should be done for the first 3 to 7 days after surgery. You can also bend your elbow and touch the shoulder on the same side a few times, then the shoulder on the opposite side a few times. And, you can raise your arms up to shoulder height or whatever is tolerable without pulling on your drains, and lower them again a few times. Breathe in as much air as you can while trying to expand your chest and abdomen (push your belly button away from your spine). This exercise will help maintain normal movement of your chest, making it easier for your lungs to work. Here are some things to keep in mind after breast surgery: q You might feel some tightness in your chest and armpit after surgery. Continuing to do some exercises during the months after surgery can help you keep good mobility. Wand exercise 33 American Cancer Society cancer. You will need a broom handle, yardstick, or other stick-like object to use as the wand in this exercise. Use your unaffected arm to help lift the wand until you feel a stretch in your affected arm. Elbow winging 34 American Cancer Society cancer. It may take many weeks of regular exercise before your elbows will get close to the bed or floor. Shoulder blade stretch 35 American Cancer Society cancer. Shoulder blade squeeze 36 American Cancer Society cancer.
Aspiration risk (neuromuscular disease erectile dysfunction pills non prescription order erectafil with a visa, gastroesophageal refux disease what causes erectile dysfunction in males erectafil 20 mg on-line, altered mental status impotent rage man cheap erectafil 20 mg online, obesity erectile dysfunction gene therapy treatment order erectafil 20mg with mastercard, pregnancy) d erectile dysfunction treatment portland oregon generic 20 mg erectafil free shipping. If risk for moderate sedation is too high erectile dysfunction age 18 order erectafil 20 mg with mastercard, consider an anesthesia consultation and general anesthesia 5. Have an emergency plan ready: Make sure qualifed backup personnel and equipment are close by 7. One provider should perform the procedure and a separate provider should monitor the patient during sedation and recovery 8. Medications to have available: Those for rapid sequence intubation (see Chapter 1) or emergencies. Continuously monitor heart rate and oxygen saturation; intermittently monitor blood pressure and respiratory rate. Airway: Assess airway patency and adequacy of ventilation through capnography, auscultation, or direct visualization frequently Chapter 6 Analgesia and Sedation 145 D. Goal of sedation: To tailor drug combination to provide levels of analgesia, sedation-hypnosis, and anxiolysis deep enough to facilitate the procedure but shallow enough to avoid loss of airway refexes 2. Data from Yaster M, Cote C, Krane E, et al: Pediatric pain management and sedation handbook. See also Tables 6-3 and 6-7 for more information on opiates and barbiturates/benzodiazepines 4. Alternatively for very young or intellectually disabled children, goal is to return as close as possible to presedation level of responsiveness 5. If no response is obtained, evaluate for other cause of sedation/respiratory depression 5. Discontinue naloxone administration: Discontinue naloxone as soon as patient responds. Caution: Another dose of naloxone may be required within 30 min of frst dose (duration of action of naloxone is shorter than that of most opioids) 7. Monitor patient: Assign a staff member to monitor sedation/respiratory status and to remind the patient to take deep breaths as necessary 8. Resume opioid administration at half the original dose when the patient is easily aroused and respiratory rate is >9 breaths/min. The reversal of analgesia could produce hypertension, tachycardia, ventricular arrhythmias, and pulmonary edema. In children younger than age 6 years, a family member, caregiver, or nurse may administer doses. Commonly used in sickle cell disease, postsurgery, post-trauma, burns, and cancer. Adapted from Yaster M, Cote C, Krane E, et al: Pediatric pain management and sedation handbook. Pruritus, nausea, constipation, urine retention, excessive drowsiness, respiratory depression 2. Conversion: Convert all drugs to a single equi-analgesic member of that group (Table 6-11) 2. Clonidine in combination with opioid has been shown to decrease the length of time needed for opioid weaning in neonatal abstinence syndrome with few short term side effects. Limited data exist evaluating use of oral clonidine in iatrogenic opioid abstinence syndrome in critically ill patients, but both transdermal clonidine and dexmedetomidine have shown promise16 c. Several studies have examined the use of clonidine in treating opioid dependence but insuffcient data exist to support its routine use outside of possibly the neonatal setting17 D. From Yaster M, Cote C, Krane E, et al: Pediatric pain management and sedation handbook. Effcacy of sweet solutions for analgesia in infants between 1 and 12 months of age: a systematic review. Preprocedural fasting state and adverse events in children undergoing procedural sedation and analgesia in a pediatric emergency department. The effects of a small-dose naloxone infusion on opioid-induced side effects and analgesia in children and Chapter 6 Analgesia and Sedation 153 adolescents treated with intravenous patient-controlled analgesia: a double blind, prospective, randomized, controlled study. Clonidine as an adjunct therapy to opioids for neonatal abstinence syndrome: a randomized, controlled trial. Four limb blood pressure measurements can be used to assess for coarctation of the aorta; pressure must be measured in both the right and left arms because of the possibility of an aberrant right subclavian artery b. Wide pulse pressure (>40 mmHg): Differential diagnosis includes aortic insuffciency, arteriovenous fstula, patent ductus arteriosus, thyrotoxicosis b. Narrow pulse pressure (<25 mmHg): Differential diagnosis includes aortic stenosis, pericardial effusion, pericardial tamponade, pericarditis, signifcant tachycardia 3. Adapted from National High Blood Pressure Education Program Working Group on High Blood Pressure in Children and Adolescents: the fourth report on the diagnosis, evaluation, and treatment of high blood pressure in children and adolescents. Midsystolic click with or without a late systolic murmur: Heard near the apex in mitral valve prolapse 3. Present in more than 80% of children sometime during childhood, most commonly beginning at age 3 to 4 years b. Likely pathologic murmur when one or more of the following are present: Symptoms; cyanosis; systolic murmur that is loud (grade 3/6), harsh, pansystolic, or long in duration; diastolic murmur; abnormal heart sounds; presence of a click; abnormally strong or weak pulses 3. Screening of Children and Adolescents5 Perform targeted screening of fasting lipid profle in children >2 years of age who fulfll one of the following criteria: 1. Parents or grandparents with premature cardiovascular disease (55 years of age for men and 65 years of age for women) 2. Parent with elevated blood cholesterol level (240 mg/dL) or other pattern of dyslipidemia Chapter 7 Cardiology 169 3. Parental history is unobtainable; particularly for those with other risk factors such as smoking, obesity/overweight, or diabetes mellitus 4. Bile acid sequestrants and statins are the usual frst-line drugs for treatment in children 4. Amplitude standard: 10 mm = 1 mV (2) Calculation: Heart rate (beats per minute) = 60 divided by the average R-R interval in seconds, or 1500 divided by the R-R interval in millimeters b. R-wave progression: There is generally a normal increase in R-wave size and decrease in S-wave size from leads V1 to V6 (with dominant S waves in right precordial leads and dominant R waves in left precordial leads), representing dominance of left ventricular forces. However, newborns and infants have a normal dominance of the right ventricle Chapter 7 Cardiology 173 g. Flat or low T waves may be seen in hypokalemia, hypothyroidism, normal newborn, and myocardial and pericardial ischemia and infammation (Table 7-5 and Fig. All patients premature and prolonged need cardiology referral depolarization of ventricles. Etiology: Anomalous origin or aberrant course of a coronary artery, Kawasaki disease, congenital heart disease (presurgical and postsurgical), and dilated cardiomyopathy. Less often associated with hypertension, lupus, myocarditis, cocaine ingestion, and use of adrenergic drugs. Diphasic T waves, seen within frst few days (becoming sharply inverted, then normalizing over time) d. Cardiac troponin I: More sensitive indicator of early myocardial damage in children. Adapted from Garson A Jr: the Electrocardiogram in Infants and Children: A Systematic Approach. Complications: Associated with the ventricular arrhythmias (torsades de pointes), syncope, and sudden death 3. Cyanotic Lesions (Table 7-13) An oxygen challenge test is used to evaluate the etiology of cyanosis in neonates. Pulse oximetry will not be useful for following the change in oxygenation once the saturations reach 100% (approximately PaO >90 mmHg). Atrial septostomy: Creates an intra-atrial opening to allow for mixing or shunting between atria of systemic and pulmonary venous blood. Most commonly performed percutaneously with a balloon-tipped catheter (Rashkind procedure) 2. Size: Cardiac shadow should be less than 50% of thoracic width (the maximal width between the inner margins of the ribs, as measured on a posteroanterior radiograph during inspiration) b. Shape: Can aid in the diagnosis of chamber/vessel enlargement and some congenital heart disease (Fig. Evaluate the trachea: Usually bends slightly to the right above the carina in normal patients with a left-sided aortic arch. Normal values range from approximately 30% to 45%, depending on age16 See more information on echocardiography on Expert Consult, Chapter 7. Common causative organisms: About 70% of causes of endocarditis are streptococcal species (Streptococcus viridans, enterococci); 20% are staphylococcal species (Staphylococcus aureus, Staphylococcus epidermidis); 10% are other organisms (Haemophilus infuenzae, gram-negative bacteria, fungi) 2. Clinical fndings: New heart murmur, recurrent fever, splenomegaly, petechiae, fatigue, Osler nodes (tender nodules at fngertips), Janeway lesions (painless hemorrhagic areas on palms or soles), splinter hemorrhages, and Roth spots (retinal hemorrhages) B. All dental procedures that involve treatment of gingival tissue or periapical region of the teeth or oral mucosal perforation 2. Invasive procedures that involve incision or biopsy of respiratory mucosa, such as tonsillectomy and adenoidectomy 3. Not recommended for genitourinary or gastrointestinal tract procedures; solely for bacterial endocarditis prevention See Table 7-15 and Box 7-4. Etiology: Infectious, toxic (alcohol, anthracyclines), metabolic (hypothyroidism, muscular dystrophy), immunologic, collagen vascular disease, nutritional defciency (kwashiorkor, beriberi) b. Echocardiography: Enlarged ventricles (increased end-diastolic and end-systolic dimensions) with little or no wall thickening; decreased shortening fraction g. Hypertrophic cardiomyopathy: Abnormality of myocardial cells leading to signifcant ventricular hypertrophy, particularly of the left ventricle, with small to normal ventricular dimensions. Increased contractile function, but impaired flling secondary to stiff ventricles. Etiology: Genetic (autosomal dominant, 60% of cases) or sporadic (40% of cases) b. Symptoms: Easy fatigability, anginal pain, shortness of breath, occasional palpitations c. Echocardiography: Extent and location of hypertrophy, obstruction, increased contractility g. Treatment: Moderate restriction of physical activity, administration of negative inotropes (-blocker, calcium channel blocker) to help improve flling and subacute bacterial endocarditis prophylaxis. Restrictive cardiomyopathy: Myocardial or endocardial disease (usually infltrative or fbrotic) resulting in stiff ventricular walls, with restriction of diastolic flling but normal contractile function. Diuretics, anticoagulants, calcium channel blockers, pacemaker for heart block, cardiac transplantation if severe 4. Variably anorexia, lethargy, emesis, lightheadedness, cold extremities, shortness of breath c. Echocardiography: Enlargement of heart chambers, impaired left ventricular function h. May require heart transplantation if no improvement (about 20% to 25% of cases) D. Symptoms: Chest pain (retrosternal or precordial, radiating to back or shoulder, pleuritic in nature, alleviated by leaning forward, aggravated by supine position), dyspnea c. Etiology: Associated with acute pericarditis (exudative fuid) or serous effusion resulting from increased capillary hydrostatic pressure. Symptoms: Can present with no symptoms, dull ache in left chest, abdominal pain, or symptoms of cardiac tamponade, discussed subsequently c. Examination: Muffed distant heart sounds, dullness to percussion of posterior left chest (secondary to atelectasis from large pericardial sac), hemodynamic signs of cardiac compression d. Echocardiography shows extent and location of hypertrophy, obstruction, increased contractility g. Observe if asymptomatic; use pericardiocentesis if there is sudden increase in volume or hemodynamic compromise. Nonsteroidal anti-infammatory drugs or steroids may be of beneft, depending on etiology 3. Cardiac tamponade: Accumulation of pericardial fuid under high pressure, causing compression of cardiac chambers, limiting flling, and decreasing stroke volume and cardiac output a. Most commonly associated with viral infection, neoplasm, uremia, and acute hemorrhage b. Examination: Jugular venous distention, hepatomegaly, peripheral edema, tachypnea, rales (from increased systemic and pulmonary venous pressure), hypotension, tachycardia, pulsus paradoxus (decrease in systolic blood pressure by >10 mmHg with each inspiration), decreased capillary refll (from decreased stroke volume and cardiac output), quiet precordium, and muffed heart sounds d. Echocardiography: Right ventricle collapse in early diastole, right atrial/ left atrial collapse in end-diastole and early systole f.