Mario Alfredo Eisenberger, M.D.
- R. Dale Hughes Professor of Oncology and Urology
- Professor of Oncology

https://www.hopkinsmedicine.org/profiles/results/directory/profile/0007314/mario-eisenberger
Aspergillus tious about accepting those types of standards in the absence of clear and Penicillium are both common medicine over the counter buy 50 mg clozaril otc. Although the test is expensive treatment 6th feb purchase clozaril paypal, there are cirduced by several different species of molds symptoms valley fever generic clozaril 50mg online, including Stachybotrys medications related to the female reproductive system discount clozaril online american express. Generally speaking medicine just for cough generic clozaril 100mg online, if you have an environmental sample that demonIn addition to carcinogenicity and mutagenicity symptoms upper respiratory infection purchase 25 mg clozaril visa, aflatoxin B1 strates the presence of trichothecenes, you can be reasonably certain causes aflatoxicoses. Chronic aflatoxicosis can involve cancer, that Stachybotrys has been in the environment. The hydrogen esters immune suppression, and various slow pathological conditions assodelineate type A from type B, and type B contains a ketone. This should be of great conion, and they are also able to interfere with protein synthesis to a sigcern to all of us. The illnesses that are associated with them can look Fumonisin B1, first described in 1988, is the most abundantly very much like radiation sickness. It is also indicatis associated with the T2 toxin, which is one of the trichothecenes. With ochratoxin, primary effects are associated with the enzymes Symptoms of the disease include inflammation of the skin, akin to St. Ochratoxin targets the accompanied by necrosis in the oral cavity, bleeding from the nose, kidney, and is also a liver toxin, immune suppressant, and a teratogen. Of all the species studied so far, humans have the longest half life for Some of these species have been looked at as antimicrobial or ochratoxin. Ochratoxin is now one of the substances that we can detect chemotherapeutic agents, but without success due to their tremenin urine and other human fluids using enzyme-linked immunosorbent dous neurotoxic effects. Ochratoxin is primarily associated with the Aspergillus Microbiology Reviews in 2003. Ochratoxin workers exposed to moldy hay, has also received attention concerning contamination of food and the presence of ochratoxin in human serums illnesses connected with the presence of Stachybotrys in building matewere more common in families with nephropathy and urinary tract rials with a high cellulose content. And ochraproduct; unlike making plywood, where the bark is stripped from the toxin is a risk factor for testicular cancer. Microscopic Patulin, a colorless, crystalline antibiotic produced by several studies of dry wall paper show that the mold spores are already there. It was reclassified as a mycotoxin and, in spite of almost all polyvinyl chloride pipe is going to deteriorate, forming litrelatively minimal data, suggested standards at the moment are for a tle pinholes that become droplet sources for water or fine sprays maximum of. The mold will then grow on the S 148 M anaging Biotransform ation: the M etabolic, Genom ic, and D etoxification Balance Points 13th International Sym posium of Gray the Institute for Functional M edicine paper on the interior of the wall. Unlike aflatoxins, triopen up a wall and, from floor to ceiling, the cavity is literally filled chothecenes can react immediately on contact, and exposure to even a with multiple species and colonies of molds. The Society for duce as much mycotoxin in the laboratory as was thought to be needOccupational and Environmental Health held a conference in ed to cause the illness. David Miller out going to produce as much mycotoxin as they do under wild condiof Canada has shown that, if you do sampling in ambient air across tions. It was also suggested that the smoking habits of the parents the continent of North America, Coelosphaerium generally predomicaused the problem. Aspergillus and Penicillium are rarely present in concentrations hemorrhagic pneumonitis, all of which were associated with greater than perhaps 1 to 2% of all molds present. When you get a Stachybotrys present in the homes and increased mold growth, he was sample in an indoor environment, and are looking for mold amplifiable to show that if you controlled for the smoking issue, the odds cation, the presence of Aspergillus and Penicillium in significant ratio was still 17:1 for increased risk of hemorrhagic pneumonitis amounts is the index. She was able to demonstrate In addition to the fact that dry wall manufacture and use have that a relationship exists. There are some data suggesting that it is not a signifilot more air flow through our buildings, still save energy, and not have cant problem, and recommendations have been made suggesting that as much moisture accumulating. Moldy grain consumption is tion of 1000 parts per million, where outdoor air is generally 250 to associated with hyperestrogenism in swine. Modern work shows that dietary concentrations of zearconcentrate all of the volatiles that are in the building by a factor of 3 alenone, as low as 1 part per million, can lead to hyperestrogenic synand still maintain our presence in these buildings. We endometrial dysplasia, endometrial cancer, and possibly endometrioshould also recognize that the potential toxicity of mycotoxins may sis. Although sick building syndrome was supposed to mean that conditions of mold amplification. It can also interact with transcription Figure 1 compares the complaints of patients in my general pracfactor and can impair glutathione metabolism, perhaps affecting tice to those of patients who had come in specifically with documentachemical sensitivity. There were One of the arguments often raised in litigation environments is allegations that the Iraqi scientists had developed aflatoxins as part of that patients are malingering. There was absolutely no statistically significant differpatients (n=297) who had documented exposure to fungus and mold. On one hand, we were seeing dramatic evidence of hyperLooking at the natural killer cell population in Figure 3, we see a activation of a variety of factors and cell types. On the other hand, cersignificant drop in the mean score for the mold-exposed patient; tain cell types and mitogen responses were decreased. Looking at lymphocyte stimulation by ly infectious agent, and the T-cell activation, in general, reflects a phytohemagglutinin (see Figure 4), the mean score expected was 145% response to potential infection by the immune system. We also looked at 13 different autoimmune markers in these remember that we need particulate sizes between 5 micron and 0. The Stachybotrys spore is 5 micron in diamemyelin were elevated in all of the patients, as compared to controls. Only 30% of the toxic Interestingly, in researching the control population, I was surprised, burden is present on the surface of the spores. Still, the odds ratios for the mold-exposed population compared times more particles and surface area involved in those sub-micron to this control group were quite substantial. Antinuclear of the action is in terms of the particulates coming from these organantibodies showed a 32% abnormal rate in this group. We see pictures of people wearing a muscle antibodies were abnormal in 33% of the group. Comparison of inflammatory responses in mouse lungs exposed to atranones A and C from Stachybotrys charthat was submerged for a week in water during hurricane Katrina in tarum. Acute pulmonary hemorrhage in infants associated with exposure to Stachybotrys atra and other fungi. American College of Governmental Industrial Hygienists, the stan1998;152(11):1055. What the Primary Care Pediatrician Should Know about Syndromes Associated with Exposures to Mycotoxins. Investigation of acute idiopathic pulmonary hemorrhage among infants Massachusetts, December 2002-June 2003. Guidance for Clinicians on the Recognition makes these organisms more mutagenic, more carcinogenic, and more and Management of Health Effects related to Mold Exposure and Moisture Indoors. Mycotoxin adducts on human serum albumin: biomarkers of exposure to Stachybotrys chartarum. Eosinophilic mucus chronic rhinosinusitis: clinical subgroups or a homogeneous pathogenic entityfi Glutathione-s-transferase M1 and T1 polymorphisms and associations with type 1 diabetes age-at-onset. Exposure to fumonisins and the occurrence of neural tube defects along the Texas-Mexico border. Genotoxicity assessment of deoxynivalenol in the Caco-2 cell line model using the Comet assay. Indoor mold, toxigenic fungi, and Stachybotrys chartarum: infectious disease perspective. Several other vitamins and minerals lead, not blood lead, is the source for lead released in sweat. When a 2-year folpatients had lower serum levels of phenytoin during a particlow-up was done, it was found that 23% of those who failed to comularly hot summer. Ron Hubbard, founder of Scientology, developed and promotChionanthus, Arctium lappa, Taraxacum, Urtica dioica, ed the use of the Hubbard Purification Rundown as a method of Arctostaphylos uva-ursi, and Silybum marianum reducing environmental chemicals in an individual. Dietary avoidance of sugar Ten electrical workers who did 3 weeks of the Hubbard protocol were studied. M anaging Biotransform ation: the M etabolic, Genom ic, and D etoxification Balance Points S 155 13th International Sym posium of the Institute for Functional M edicine Crinnion 8. Repeated sauna treatment improves vascular endothelial function in patients with chronic heart failure. Thermal hydrotherapy improves quality of life and hemodynamic function in patients with Autoimmune 0 0 0 4 12 16 chronic heart failure. Effects of repeated sauna treatment on ventricular 6 15 arrhythmias in patients with chronic heart failure. Atomic absorption General Cleansing 0 0 2 5 spectrometry of nickel, copper, zinc and lead in sweat collected from healthy subjects during sauna bathing. A comparative study of copper, lead, cadmium and zinc in Dermatological 0 0 0 3 1 4 human sweat and blood. Lead in sweat and its relationship to salivary and urinary levels in normal healthy subjects. When saunas are used to reduce blood pressure and chlorobenzene and polychlorinated biphenyls. Reduction of chemical enhance blood flow and cardiac functioning, only short sauna sessensitivity by means of heat depuration, physical therapy and nutritional supplesions (15 minutes) are necessary. Presentation at the American Academy of Environmental Medicine annual scientific session. Results of a decade of naturopathic treatment for environmental illeither use, saunas are safe and effective and should be used more frenesses. Sauna therapy in coronary heart disease with hypertension after bypass operation, in heart aneurysm operation and in essential hypertension. Changes of central and peripheral hemodynamics during isometric and dynamic exercise in hypertensive patients before and after regular sauna therapy. Mathias Plauth Klinik fur Innere Medizin Stadtisches Klinikum Dessau Auenweg 38 06847 Dessau Germany Editorial section for practical dietetics S. Cirrhosis of the liver (liver shrinkage), which is characterized by the progressive destruction of liver cells, can be slowed by correct eating and drinking. Diet in cirrhosis of the liver and other chronic liver diseases does not mean skimmed quark by the pound or a bland diet that is low in fat and lacking in taste! The recipes are preceded by a detailed and clear medical introduction and dietetic information. The hepatic artery brings oxygen-rich blood to the liver while the portal vein transports nutrient-rich blood to the liver. The blood in the portal vein has already passed through the gastrointestinal tract and absorbed large amounts of nutrients. Proteins are also required for the performance of bodily functions, such as muscle contractions and the production of antibodies to defend against invading microbes.
However medicine 1950 discount clozaril on line, a urethral injury should be suspected in any patient with a pelvic fracture or significant trauma to the perineum until confirmed otherwise by a diagnostic work-up symptoms 37 weeks pregnant cheap clozaril express. Signs of urethral injury are blood at the meatus medications zetia discount 50mg clozaril mastercard, gross haematuria medications you cant take while breastfeeding purchase 50 mg clozaril overnight delivery, and pain during voiding or an inability to void medicine you can order online order 25mg clozaril with amex. A rectal examination to determine the position and fixation of the prostate is important in any male with a suspected urethral injury symptoms 7 days after embryo transfer 50 mg clozaril overnight delivery. The prostate, as well as the bladder, may be displaced up out of the pelvis, especially in membranous urethral trauma. If a catheter has already been placed by someone else and there is suspected urethral trauma, the catheter should be left in place and should not be removed. Instead, a small infant feeding tube can be placed into the distal urethra along the catheter to allow the injection of contrast material for a diagnostic scan [748]. A transurethral catheter should only be inserted if there is a history of voiding after the traumatic event, and if a rectal and pelvic examination, as described above, has not suggested a urethral rupture. If the catheter does not pass easily, an immediate retrograde urethrogram should be performed. A suprapubic tube may be placed in the emergency department percutaneously, or even in the operating room, if the patient has to undergo immediate exploration because of other life-threateninginjuries. There are often no associated injuries with a bulbous urethral or straddle injury and management is therefore usually straightforward. In these cases, a transurethral catheter is the best option for preventing urethral bleeding and/or painful voiding [749]. The initial management of posterior urethral injuries remains controversial, mainly regarding the long-term results with primary realignment compared to simple suprapubic drainage with later reconstruction. Suprapubic drainage and late urethral reconstruction was first attempted because immediate surgical repair had a poor outcome, with significant bleeding and high rates of incontinence (21%) and impotence in up to 56% of cases [750]. In adults, a study of the success rates of delayed repair reported re-structure rates of 11-30%, continence rates of 90-95% and impotence rates of 62-68% [751]. The largest paediatric series of delayed repair in 68 boys reported a success rate of 90% [752]. Another study reported strictures and impotence in 67% of boys, although all the boys were continent [751]. An alternative to providing initial suprapubic drainage and delayed repair is primary realignment of the urethra via a catheter. The catheter is usually put in place during open cystostomy by passing it from either the bladder neck or meatus and through the injured segment. B Bulbous urethral injuries can usually be managed conservatively with a transurethral catheter. B There is still controversy about the optimal management for posterior urethral disruption. The options C include primary reconstruction; primary drainage with a suprapubic catheter alone and delayed repair; primary re-alignment with a transurethral catheter. Compared to adults, children have a different total body fluid distribution, renal physiology and electrolyte requirements, as well as weaker cardiovascular compensation mechanisms [754]. As children are developing, they have a high metabolic rate and low fat and nutrient stores, which means they are more susceptible to metabolic disturbances caused by surgical stress [755]. The metabolic response to anaesthesia and surgery in infants and children is related to the severity of the operation [756]. Table 14 gives the current guidelines for pre-operative fasting for elective surgery [757, 758]. Table 14: Pre-operative fasting times for elective surgery Ingested material Minimum fasting period (h) Clear liquids 2 Breast milk 4 Infant formula 4 (< 3 months old) to 6 (> 3 months old) Non-human milk 6 Light meal 6 Although hypoglycaemia is an important issue in children, research has shown that hypoglycaemia is uncommon if children are still fed up to 4 h before the induction of anaesthesia [759]. Newborns often have low glycogen stores and impaired gluconeogenesis, both of which can be helped by limiting the period of preoperative starvation and feeding with glucose-containing solutions. It is important to monitor blood glucose and to adjust the glucose supply continuously in neonates and those children who are small for their age, as this helps to prevent excessive fluctuation in blood glucose levels [760]. The goal of intra-operative fluid management is to sustain homeostasis by providing the appropriate amount of parenteral fluid; this maintains adequate intravascular volume, cardiac output and oxygen delivery to tissues at a time when normal physiological functions have been altered by surgical stress and anaesthetic agents [760]. The fluids for maintenance therapy replace losses from two sources: insensible (evaporation) and urinary loss. They do not replace blood loss or third-space fluid loss into the interstitial space or gut. The main formulae for calculating the daily maintenance requirement for water have not changed in the past 50 years (Table 15) [761]. Calculations have shown that anaesthetised and non-anaesthetised children have similar fluid requirements [762]. The usual intravenous maintenance fluid given to children by paediatricians is one-quarter to one-third strength saline [763]. Table 15: Hourly and daily fluid requirements according to body weight Body weight Hourly Daily < 10 kg 4 mL/kg 100 mL/kg 10-20 kg 40 mL + 2 mL/kg; > 10 kg 1000 mL + 50 mL/kg; > 10 kg > 20 kg 60 mL + 1 mL/kg; > 20 kg 1500 mL+ 20 mL/kg; > 20 kg the fasting deficit is calculated by multiplying the hourly maintenance fluid requirement by the number of hours of fluid restriction. It is recommended that 50% of the fasting deficit is replaced in the first hour and 25% in the second and third hours [764]. Five percent dextrose with one-quarterto half-normal saline is often used as a maintenance fluid, while balanced salt solution or normal saline is used as replacement fluid. Blood losses are replaced with a 1:1 ratio of blood or colloid or a 3:1 ratio of crystalloid. If appropriate, albumin, plasma, synthetic colloids, and blood should be administered [760]. Third-space losses may vary from 1 mL/kg/h for a minor surgical procedure to 15-20 mL/kg/h for major abdominal procedures, or even up to 50 mL/kg/h for surgery of necrotising enterocolitis in premature infants. Most of the fluids required during surgery are needed to replace fasting deficit or third-space losses, which are mainly extracellular fluids. Hydrating solutions should contain high concentrations of sodium and chloride and low concentrations of bicarbonate, calcium and potassium. In contrast, hyperglycaemia is commonly encountered during anaesthesia and surgery. The replacement fluid should be free of dextrose or should not have > 1% dextrose. Current recommendations include the use of low-dextrose-containing solutions for maintenance fluid therapy, except in patients who are at high risk of hypoglycaemia [754, 763]. Intra-operative administration of glucose-free isotonic hydrating solutions should be the routine practice for most procedures in children over 4-5 years of age. In minor surgical procedures, intra-operative administration of large volumes of crystalloids is associated with a reduced incidence of post-operative nausea and vomiting after anaesthesia in both paediatric and adult patients [767]. It is not obligatory to check serum chemistry after uncomplicated surgery in children with normal pre-operative renal and hepatic function. Post-operative findings, such as decreased bowel movements and ileus, may be signs of hypokalemia, which may be corrected with a solution of 20 mmol/L potassium and an infusion rate of not more than 3 mmol/kg/day. The potassium should be given via peripheral venous access if the duration of infusion is not expected to exceed 5 days, or via central venous access when long-term parenteral nutrition is necessary. The goals of fluid therapy are to provide basic metabolic requirements and to compensate for gastrointestinal and additional losses. Hyponatremia is the most frequent electrolyte disorder in the post-operative period [768, 769]. This means that hypotonic fluid should not be routinely administered to hospitalised children because they have several stimuli for producing arginine vasopressin and are therefore at high risk for developing hyponatremia [758, 768, 770-773]. It is also advisable to administer isotonic fluids intra-operatively and also immediately post-operatively, albeit at two-thirds of the calculated maintenance rate in the recovery room. Fluid composition should balance high sodium requirements, energy requirements and solution osmolarity. Fluid that has been given to dilute medications must also be taken into account [758]. Children who undergo interventions to relieve any kind of obstructive diseases deserve particular attention, especially the risk of polyuria due to post-obstructive diuresis. In children who develop polyuria, it is important to monitor fluid intake and urine output, as well as renal function and serum electrolytes. If necessary, clinicians should not hesitate in consulting with a paediatric nephrologist. However, a study found that if children were freely allowed to drink and eat when they felt ready or requested it, the incidence of vomiting did not increase and the children felt happier and were significantly less bothered by pain than children who were fasting [776]. The mean times until first drink and first eating in the children who were free to eat or drink were 108 and 270 min, respectively, which were 4 h and 3 h earlier than in the fasting group. Previous studies have suggested that gastric motility returns to normal 1 h after emergence from anaesthesia in children who have undergone non-abdominal surgery [777]. The first oral intake in children at 1 h after emergence from anaesthesia for minor surgery did not cause an increase in the incidence of vomiting, provided that the fluid ingested was at body temperature [778]. They have their own unique metabolic 2 features, which must be considered during surgery. B Care should be taken for hyperglycaemia, which is common in children, compared to intra-operative B hypoglycaemia, which is very rare. Avoid the routine use of hypotonic fluid in hospitalised children because they are at high risk of A developing hyponatremia. It is therefore B essential to measure the baseline and daily levels of serum electrolytes, glucose, urea and/or creatinine in every child who receives intravenous fluids, especially in intestinal surgery. In patients treated with minor surgical procedures, early oral fluid intake should be encouraged. However, there is still no standardised algorithm for management of post-operative pain in children [780]. There is an urgent need for a post-operative pain management protocol in children, particularly for guidance on the frequency of pain assessment, use of parenteral opioids, introduction of regional anaesthesia, and the application of rescue analgesics [781]. Traditional medical beliefs that neonates are incapable of experiencing pain have now been abandoned following recent and better understanding of how the pain system matures in humans, better pain assessment methods and a knowledge of the clinical consequences of pain in neonates [782-786]. Many studies have indicated that deficient or insufficient analgesia may be the cause of future behavioural and somatic sequelae [787-791]. Our current understanding of pain management in children depends fully on the belief that all children, irrespective of age, deserve adequate treatment. Validated pain assessment tools are needed for this purpose and it is important to select the appropriate pain assessment technique. One of the most important topics in paediatric pain management is informing and involving the child and parents during this process. Parents and patients can manage post-operative pain at home or in hospital if provided with the correct information. Parents and patients, if they are old enough, can actively take part in pain management in patient-family-controlled analgesia applications [794-799]. Local anaesthetics or non-steroidal analgesics are given intra-operatively to delay post-operative pain and to decrease post-operative analgesic consumption. Opioids can be administered to children by the oral, mucosal, transdermal, subcutaneous, intramuscular or intravenous routes [796]. The same combination of local anaesthetics, opioids, and non-opioid drugs used in adults can also be used in children taking into account their age, body weight and individual medical status. Post-operative management should be based on sufficient intra-operative pre-emptive analgesia with regional or caudal blockade followed by balanced analgesia. As they become insufficient to prevent pain, weak and strong opioids are added to oral drugs to achieve balanced analgesia. Mogen clamp), a pacifier, sucrose, and swaddling, preferably in combination [805-809]. Ultrasonographic guidance may improve the results, with an increase in procedural time [811, 812]. However, parents should be informed about the more frequent incidence of post-operative motor weakness and micturition problems [813-818]. Several agents with different doses, concentrations and administration techniques have been used with similar outcomes [819833]. Both single and combined use of these agents is effective [820, 821, 823, 824, 829, 831]. Penile blocks can be used for post-operative analgesia and have similar post-operative analgesic properties as caudal blocks [834]. Two penile blocks at the beginning and end of surgery seems to provide better pain relief [835]. Severe bladder spasms caused by the presence of the bladder catheter may sometimes cause more problems than pain and is managed with antimuscarinic medications. For inguinoscrotal surgery, all anaesthetic methods, such as caudal blocks [307, 836-838], nerve block [839, 840], wound infiltration or instillation, and irrigation with local anaesthetics [841-843], have been shown to have adequate post-operative analgesic properties.
For several decades before the therapeutic triumph of Minot and Murphy treatment 2015 purchase cheap clozaril on-line, it was known that patients with pernicious anemia had severe atrophy of the gastric mucosa symptoms 3 days before period buy generic clozaril 50 mg. Also medicine nobel prize 2015 generic clozaril 25mg without a prescription, their gastric juices were known to be scanty and lacking in acid and peptic activity symptoms non hodgkins lymphoma purchase clozaril 50mg overnight delivery. William Castle postulated that the gastric pathology might be playing a causal role in pernicious anemia symptoms 6 days after iui order clozaril from india, and he proved his postulate with brilliantly conceived and controlled therapeutic trials alternative medicine 100mg clozaril free shipping. During the next ten days, however, he fed the patient the same quantity of hamburger with normal human gastric juice, and generated an impressive reticulocyte response, increase in hemoglobin and sense of well-being. The identification of the anti-pernicious-anemia principle in liver had to wait until 1948. In that year, scientists at American and British pharmaceutical firms simultaneously and independently reported the isolation and crystallization of vitamin B12. Each of these groups had demonstrated that the crystallized vitamin was extremely effective in the treatment of pernicious anemia. The first reports showed that, on one occasion, the injection of as little as ten micrograms of vitamin B12 led to a significant hematologic improvement. It was soon demonstrated that the red vitamin (so named because of its deep red color) contained cobalt bound into a tetrapyrrole ring, somewhat analogous to the iron in heme. A second Nobel prize related to vitamin B12 was awarded to Dorothy Hodgkin for her X-ray crystallographic studies demonstrating the exact structure of the vitamin (molecular weight 1,350 daltons), as diagrammed in Figure 3. Commercial vitamin B12 is derived from microbial synthesis, an efficient and inexpensive process compared to chemical synthesis; a quantity sufficient to treat a pernicious anemia patient for a whole year costs no more than a few dollars. Physiology the typical daily Western diet contains five to thirty micrograms (fig) of vitamin B12 in animal, bird and fish products, of which the liver and kidney are especially rich sources. Their function in the gut is unknown but it has been speculated that they help dispose of inactive cobalamin analogues. In the absence of intrinsic factor, only one to two percent of B12 is absorbed, but with intrinsic factor, 60-90% of a test dose of aqueous B12 will be absorbed. It is likely that megaloblastic anemia and neurologic disease due to vitamin B12 deficiency occur after body stores of the vitamin have decreased to less than 20% of normal. Biochemistry Cyanocobalamin, a stable form of vitamin B12 was the first cobalt-containing organic compound shown to have a biologic role. Students of animal husbandry knew that cobalt was an essential nutrient for sheep. After isolation, crystallization and partial characterization of cyanocobalamin from liver in 1948, the role of cobalt in the maintenance of life of all animals and many bacteria began to emerge. In mammals, only two reactions clearly requiring vitamin B12 have been identified. The reversible conversion of methylmalonyl CoA to succinyl CoA is catalyzed by methylmalonyl CoA mutase, which requires adenosylcobalamin as a cofactor (Fig. Deficient activity of methylmalonyl CoA mutase is thought by some investigators to be the cause of the neurologic disease in B12 deficiency. The methylation of homocysteine to form methionine requires enzyme-bound 5 methylcobalamin and N methyltetrahydrofolate as a methyl donor (Fig. Methionine provides a methyl group for modification of myelin basic protein; a deficiency of methionine is believed by some to decrease synthesis of myelin, leading to demyelination of the posterior and lateral columns of the spinal cord. However, since homocysteine accumulation in serum is regularly seen in folate deficiency as well as in B12 deficiency, the failure of this enzyme reaction does not explain the extreme rarity of neurologic disease in folate deficiency and the frequency of neurologic disease in cobalamin deficiency. Linkage of folate and cobalamin in the methylation of homocysteine to form methionine. The interdependence of vitamin B12 and folate in this methyl transfer is shown schematically in Figure 3. There is evidence that the sera of vitamin B12-deficient patients contain higher than expected levels of methyltetrahydrofolate. Thus, it appears that B12 deficiency leads to a functional folate deficiency in dividing cells. If intracellular folate deficiency is the common lesion in B12 and folate deficiency, the morphologic identity of the megaloblastic abnormalities in these two conditions is understandable. Mechanisms of Vitamin B12 Deficiency the most common cause of B12 deficiency in the Western world is an acquired loss of intrinsic factor, also known as "pernicious anemia. Parietal cells may be lost by autoimmune destruction of the gastric mucosa, by physical or chemical injury, or by surgical removal. Autoimmune destruction of gastric parietal cells is far and away the most common cause of B12 deficiency. The risk of vitamin B12 deficiency from inadequate intake is greatest in strict vegans, who eat neither eggs nor milk products. There are few true vegans in the United States, so dietary insufficiency is rarely a cause of megaloblastic anemia. Because B12 is avidly taken up and biochemically altered by many microorganisms, one might expect some patients with small intestinal disease accompanied by massive bacterial overgrowth to suffer from B12 malabsorption and deficiency. This is the case in several anatomic and physiologic disorders of the gut, especially large diverticula of the small intestine or a surgically created blind loop (hence the term "blind loop syndrome"). Anaerobic organisms such as Bacteroides avidly bind vitamin B12, even when it is coupled to intrinsic factor, 55 rendering the vitamin unavailable for absorption. Fish tapeworm infestation is common in Finland, and B12 deficiency often follows because the worm is a successful competitor for B12. The pancreas also plays a role in B12 absorption; patients with extensive chronic pancreatitis or with cystic fibrosis often fail to absorb B12 when given an oral test dose. The malabsorption is corrected by the simultaneous oral administration of pancreatic extract or trypsin. At the ileum, B12 is transferred from its intrinsic factor complex into the circulation and cells of the body. Thus, structural injury to the gastrointestinal tract (destruction of the gastric mucosa, injury to the pancreas, blind loop or giant diverticulae of the small intestine, or destruction of the ileum) leads to B12 deficiency more commonly than dietary nutritional deficiency or genetic metabolic derangement. The use of nitrous oxide for anesthesia in unrecognized subclinical B12 deficiency has led to severe neuropathy. Recreational abuse of nitrous oxide has led to macrocytosis and neuropathy indistinguishable from B12 deficiency. Nitrous oxide reduces the activity of methionine synthetase probably by inactivating the B12 coenzyme portion of the molecule. Pernicious Anemia A formal definition of pernicious anemia is autoimmune or idiopathic gastric atrophy sufficient to cause vitamin B12 malabsorption due to lack of intrinsic factor. Serology Sera from most patients with pernicious anemia contain autoantibodies to gastric parietal cells, but these antibodies have low specificity. Anti-parietal cell antibodies are relatively common in patients with other autoimmune diseases such as myxedema, diabetes, and gastritis. Autoantibodies to intrinsic factor are present in only about 60% to 70% of sera from patients with pernicious anemia, but they have high specificity. The presence of intrinsic factor antibodies is almost diagnostic of "pernicious anemia. The failure to absorb vitamin B12 is permanent in patients with pernicious anemia, who must receive supplemental B12 for life. Vitamin B12 deficiency is a disease of the second half of life, the incidence being roughly one new case per year per 4,000 people over 40 years of age. There also is a hereditary form of lack of functional intrinsic factor, known as "juvenile pernicious anemia. In addition to the usual physical findings of anemia, the pernicious anemia patient may complain of a sore tongue, which is often smooth, red, and glistening due to lack of papillae. The tongue symptoms and appearance will improve promptly after the correction of the vitamin B12 deficiency. Patients may complain of paresthesias and difficulty walking in the dark, and may appear neurotic. Neurologic examination will often reveal absence of vibratory sensation and proprioception. Individuals with mild to moderate neurologic deficits can be expected to make a complete recovery following B12 therapy, though the time required to recover full function may be as much as twelve to sixteen months. Recovery from advanced neurologic damage (inability to walk, incontinence) is unlikely to be complete. Neurologic disease in a person with megaloblastic anemia is highly suggestive of B12 deficiency rather than folate deficiency. In some patients, the neurologic disease is prominent with little or no anemia, while others have prominent anemia with normal neurologic examinations. If a patient with B12 deficiency is mistakenly treated with folate, neurologic disease may progress to irreversible crippling. Degeneration of the posterior and lateral columns of the spinal cord in vitamin B12 deficiency. Pancytopenia (decreased red cell, platelet, and granulocyte production) may occur in severe deficiency. Macrocytosis and dissociation of maturation in nucleus and cytoplasm have also been described in cells from other rapidly growing tissues such as skin, tongue, testis, bronchus, stomach, and cervix. There are cases of infants who became B12 deficient while nursing from mothers who were strict vegans or who had gastric bypass for obesity. Red cell destruction is mainly in the marrow rather than in the blood (see chapter 2). The erythroid marrow is hypercellular with a 1:1 G:E ratio, and the total marrow mass is greatly increased. The Schilling Test the most common cause of B12 deficiency is malabsorption rather than dietary deficiency. There are several different mechanisms of B12 malabsorption, and a radioactive B12 absorption study is a procedure to sort them out. Though no longer used clinically, it elucidates the pathophysiology of B12 deficiency. The urine radioactivity test (Schilling Test) was developed to measure B12 absorption. Radioactivity appearing in the urine after an oral dose of radioactive B12 represents absorbed vitamin. Because absorbed B12 is normally bound to plasma transcobalamins, no radioactive vitamin is filtered at the glomerulus (molecular weight of B12 is 1,350 daltons). Serum B12 concentration should be measured in all patients with dementia and neuropathy, so that this treatable cause of serious neurologic disease is not overlooked. Measurements of serum homocysteine and methylmalonate are useful in defining metabolic evidence of cobalamin deficiency. One should bear in mind that as tests for clinically significant cobalamin deficiency, these measurements appear to have excellent sensitivity but poor specificity. Treatment of B-12 deficiency fi Vitamin B12 is used to treat or prevent deficiency, usually given parenterally. History Within a few years after the demonstration of the remarkable efficacy of liver in the treatment of pernicious anemia, it was realized that not all megaloblastic anemia was due to a deficiency of the factor present in injectable liver extract. She demonstrated in a convincing manner that injections of purified liver extract (so wonderfully efficacious in pernicious anemia in London) did not benefit the megaloblastic anemia of pregnancy in Bombay. She did find that eating generous amounts of "marmite" (a yeast extract) led to impressive hematologic and subjective improvement. From this observation came the term "Wills Factor" to identify that beneficial nutrient in yeast. In 1946 folic acid was identified and synthesized by scientists at Lederle Laboratories studying growth factors for certain bacteria. Yeast is the richest nonmedicinal source of folate, but many vegetables, dairy products, and seafoods are excellent dietary sources. Food folate found in spinach, beans, broccoli, and other green leafy vegetables is in the polyglutamate form. An intestinal brush border deconjugase cleaves all but the last glutamate and thus enhances absorption. The biologic half-life of folic acid is less than one month, in contrast to the 18 month half-life of vitamin B12. For example, the methylation of deoxyuridine monophosphate to deoxythymidine monophosphate is catalyzed by thymidylate synthetase in a reaction linked to dihydrofolate reductase. Other reactions requiring folic acid coenzymes are serine conversion to glycine, histidine catabolism, methionine synthesis from homocysteine, and purine synthesis. Inadequate diet Diets composed exclusively of tea and toast or brandy and beer rapidly lead to folate deficiency. Food folate can be lost because it is easily oxidized when vegetables are cooked in boiling water. One physician investigator intentionally induced folic acid deficiency in himself in three months merely by thoroughly boiling his food and discarding the water.
Syndromes
- Creation of an opening (stoma) in which urine flows into a special pouch (this is called urinary diversion)
- Cytology exam of pleural fluid
- 24 hours: 8 - 25%
- Depression
- Mouth ulcers
- Systemic lupus erythematosus
- Your genes
- Washing of the skin (irrigation) -- perhaps every few hours for several days
- Vomiting
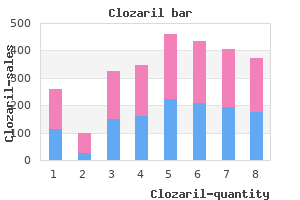
These kinds of products treatment xanthelasma cheap clozaril 100mg without a prescription, as well as dietary suppopulation symptoms 4dpiui cheap clozaril 25mg free shipping, as well as the frequency and amount of plements medicine cat herbs effective clozaril 50 mg, appear to be a reasonable way to proceed consumption by individuals medicine cabinets with lights purchase clozaril 100 mg line. If those conditions are to reduce iron deficiency anemia in developing not fulfilled symptoms panic attack purchase clozaril 25 mg without prescription, then targeted fortification and dietary countries medications band order genuine clozaril line. Inspection In developing countries, mass fortification may should be based on sensible standards that reflect still be the most cost-effective strategy to bridge the variation of the process, and micronutrient decay nutritional gap for essential micronutrients other during the marketing time of the food and when than iron. Howalso implement quality control and auditing proever, it is important to emphasize that the technocedures, based on checking one or very few logical feasibility of mass fortification is linked to micronutrients. In order that such a system works, foods produced by centralized and adequately the quality of the micronutrient mixes and predeveloped industries. Cavalli-Sforza T, Berger J, Smitasiri S, Viteri Garby L, Rossander L, Plee-hachinda R, Suwanik R, F. Absorption from iron tablets given women of reproductive age: Impact, overview, leswith different types of meals. The reduction and encapsulation affect the bioavailabiliusefulness of elemental iron for cereal flour ty of ferric pyrophosphate in rats. Dual fortification of tti) fortified with vitamin A and iron in improving salt with iodine and microencapsulated iron: a ranvitamin A and iron status in healthy, school aged domized, double-blind, controlled trial in Moroccan children in rural Bangladesh. The use of iron-fortified wheat flour to reduce controlling iron deficiency: a population-based anemia among the estate population in Sri Lanka. Brian is an advocate for the adoption of socially constructive development policies. The scale and magnitude of the adequate and varied diet in combination with the problem combined with the functional impact use of supplements and fortification strategies such deficiencies have on the quality of life, both rather than through the use of supplements or forphysiologically and socioeconomically, require tification strategies alone. This is in keeping with the urgent adoption of known and effective measthe right to food, a concept whose achievement ures. However, the focus of development practimeans that all people should be able to gain tioners on their own narrow area of interest or access to a varied diet consisting of a variety of expertise, be it health care or food, has prevented foods that provide all the energy and macroand the realization of a truly comprehensive approach micronutrients sufficient to achieve a healthy and being taken to tackle this critical problem. Iron is reversibly stored within the liver as needs and dietary diversity continues to be the ferritin and hemosiderin and is transported major challenge. Consequently, efforts to reduce between different compartments in the body by micronutrient malnutrition need to be placed in the protein transferrin. However, the sensitivity and specificity of the underlying causes of such high levels of these indicators is unclear and a combination of malnutrition, including the high levels of microthese indicators is sometimes used. This occurs at a serum ferquality, and variety of foods for all population ritin level <15 mg/L. The A requirement is an intake level which meets concentration of transferrin in plasma increases in specified criteria of adequacy while preventing an effort to compensate. Nutritional anemia is a condition in which the hemoglobin content of blood is lower than A food-based strategy has the goal of normal as a result of a deficiency of one or more improving nutrition through increasing the avaiessential nutrients. Because anemia is the most lability and consumption of a nutritionally adecommon indicator used to screen for iron defiquate micronutrient rich diet made up of a variety ciency, the terms anemia, iron deficiency, and of available foods. The prevalence of all people, at all times, have physical, social and iron deficiency anemia is therefore less frequent economic access to sufficient, safe, and nutritious than iron deficiency. Iron deficiency anemia is a food that meets their dietary needs and food prerather imprecise concept and has no immediate ferences for an active and healthy life. The main benefit of using cut-offs is mated at 14 mg/kg body weight/day with a nonto allow comparisons to be made between populamenstruating 55-kg woman losing about 0. Thompson Requirements for iron vary depending on age, tates, polyphenols, calcium, and phosphate) are physiological status, growth rate, degree of physfound in bran products, bread made from high ical maturity, body composition, and activity extraction flour, breakfast cereals, oats, rice level. Increased requirements are also noted in (especially unpolished rice), pasta products, patients with malaria, congenital hemoglococoa, nuts, soya beans, and peas; iron-binding binopathies, and other causes of hemolysis. In infant foods containing soy proteins, the explained below, it is only possible to meet these inhibiting effect can be overcome by the addition high requirements if the diet has a consistently of sufficient amounts of ascorbic acid. Consumphigh content of meat and foods rich in ascorbic tion of betel leaves, common in areas of Asia, also acid. However, again the addition of certain vegetables Iron is present in foods in two forms, as heme or fruits containing ascorbic acid can double or iron, which is derived from flesh foods (meats, triple iron absorption thereby counteracting many poultry, and fish), and as non-heme iron, which is of the effects of these inhibitors depending on the the inorganic form present in plant foods such as other properties of the meal. As the effect is so cereals, pulses, legumes, grains, nuts, and vegetamarked, this may be considered as one of vitamin bles. Each meal should prefeabsorption of heme iron from meat-containing rably contain at least 25 mg of ascorbic acid and meals of around 25%, ranging from about 40% possibly more if the meal contains many during iron deficiency to about 10% when iron inhibitors of iron absorption. Just the addition of certain quently, the amount of iron absorbed not only spices. Therefore to a marked degree, on the composition of the to translate physiological iron requirements into meal. A study on the bioavailabilkeep iron in the ferrous form) need to be present ity of different Indian diets found 1. These enhancing factors iron was absorbed from millet-based diets, include ascorbic and citric acids found in certain 3. Other studies from South bles; cysteine-containing peptides found in meat, East Asia show absorption rates can rise significhicken, fish, and other seafood; and ethanol and cantly from less than 5% to more than 15% if fermentation products like vegetables, soy sauce, animal products and vitamin C are amply proetc. Other foods contain factors for iron at four levels of dietary iron bioavailabil(ligands) that strongly bind ferrous ions and ity (5, 10, 12 and 15%) and are given in Table inhibit absorption. In nonpathological states the Recommended Food-based approaches for combating iron deficiency 341 Table 20. This is especially true if there are iron absorption inhibitors in the diet such as phytate or tannins. Among children the determiare slightly lower (20 mg) due to variation in nants of iron deficiency anemia are age (the body size. In premenopausal women aged younger the child, the higher the risk with the between 19 and 50 the recommended intake is weaning period in infants being especially critical 59 mg (2). Among pregnant women the determiiron stores are replenished), and by the properties nants are age, gravida, and stage of gestation with of the meal as determined by the amount of heme women below 20 years of age, those who have and non-heme iron in the meal, food preparation been pregnant before, and those in their second practices in terms of cooking time and temperaand third trimester being more prone to defiture, and the presence of enhancing dietary facciency. Among lactating women the determinants tors such as meat peptides and vitamin C, and are period of lactation and vitamin A status. In Iron deficiency and iron deficiency anemia are India, the National Family Health Survey worldwide public health problems. Low levels of plasma iron, folate, zinc, and In many developing countries, anemia rates in vitamins B12 and A have also been shown to be children are high (above 50%) and the severity of associated with anemia. These cognitive effects are a have a significant impact on human welfare strong argument for the more active and effecboth at the level of the individual and for the tive combating of iron deficiency, especially in economic development of a country. At the women up through the period of adolescence individual level, iron deficiency has several and into early adulthood prior to and during negative effects on important functions of the pregnancy, and for infants and children. Deficiency can slow growth, hinder physical and mental development, and reduce Iron deficiency negatively influences the the ability of the body to maintain itself. The cell-mediated lowered resistance to infection and increased immunologic response of T lymphocytes is morbidity and mortality rates, adverse pregim-paired as a result of a reduction in the fornancy outcome, and reduced school performation of these cells. There is a relationship increases the dangers of lead poisoning, partieven with mild iron deficiency and brain cularly among young children. Studies have found indicators of iron status associated with a number of cognitive Iron deficiency reduces the physical abilities in young school children, and with capacity to do work, which seems to be less 344 B. Thompson related to the degree of anemia than to the Factors that determine iron deficiency anemia impaired oxidative metabolism in the muscles due include overall low incomes and poverty that to the lack of iron-containing rate-limiting enzymes result in low overall food intakes and poor monotfor oxidative metabolism. Poor dietary intake both in terms of total Since the highest prevalence is found in quantity of food and of micronutrient rich food infants, children, adolescents, and women of are often the major cause of micronutrient malnuchildbearing age, the burden falls not just on the trition. The debilican satisfy the nutritional needs of population tating consequences include loss of human capital groups so long as the capacity to produce and purand reduced work capacity and therefore of prochase food is not limited for example by socioductivity in adults. Does this ble resource-poor subsistence farmers and landimply that the normal diet cannot cover physiologiless laborers whose main food supplies come cal iron requirementsfi For many years nutritionists directly from the land and who often have have assumed that all nutrients can be obtained restricted access to fortified foods due to low purfrom a diet containing a variety of foods drawn chasing power and undeveloped distribution from a variety of sources. Those who are physiologically vulnerapeople had access to a sufficient quantity and varible include those groups with special dietary ety of foods, then they would meet their nutritional problems or nutritional needs, including women needs. This still may be true, but despite increases of childbearing age, pregnant and lactating in the availability of a wide variety of foods in women, young children and famine-affected popalmost every country in the world, the continued ulations, who may lack access to a diet that is sufexistence of micronutrient deficiencies, including ficient in quantity or quality to provide adequate iron deficiency anemia, throws this general levels of iron. Why have improved food the food and nutrition needs of both these vulnersupplies not necessarily resulted in adequate vitaable groups. Food-based approaches for combating iron deficiency 345 Iron requirements also tend to be difficult to not possible. As demonstrated in the analysis of meet, and replenishment remains challenging for typical staple-based diets, micronutrient rich those severely deficient. Low bioavailability of foods including small amount of flesh foods and a iron in cerealand tuber-based diets is one of the variety of plant foods (vegetables and fruits) are main causes of iron deficiency anemia in low needed daily. This may not be realistic at present income countries, as they contain high amounts of for many communities living under conditions of polyphenols (tannins) and phytates that inhibit poverty. Anumber of practical actions and tion are important alternatives that complement interventions that can reduce these effects are prefood-based approaches to satisfy the nutritional sented below. A number of potential dietary sources need to be urgently promoted including many leafy vegePoor monotonous diets deficient in one mitables and legumes that contain important quanticronutrient are also likely to be deficient in other ties of iron, with special emphasis on increasing micronutrients, as well as in other important the consumption of animal products that are high foods such as fat and protein that further reduce in bioavailable iron and in iron absorption absorption of what nutrients have been ingested, enhancers. Population groups consuming such intake in children under 3 years of age was posidiets are known to have multiple micronutrient tively related to hemoglobin, suggesting low meat deficiencies. At the same time, increasing the consumption of a greater variety of plant foods, especially of the addition of small quantities of particular fruits and vegetables, will provide most of the foods to a cerealor tuber-based diet increases the missing vitamins and minerals. The addition of number of plant-based nutrients or phytochemilegumes can slightly improve the iron content of cals will be consumed and there is emerging evicerealand tuber-based diets. However, the dence on the health benefits from food phytobioavailability of this non-heme iron source is chemicals. Therefore, it is not possible to meet the revariety of foods could play a major role in offsetcommended levels of iron from staple-based diets ting what is called the double burden of malnutriunless some meat, poultry, or fish is included. Adding 50 g of meat, poultry, or fish increases total iron content as well as the amount of bioavailable iron. Rice 598g Rice 590g Rice 570g Rice 483g Rice 477g Rice 468g Rice 428g Veg oil 25g Veg oil 25g Veg oil 25g Veg oil 25g Veg oil 25g Veg oil 25g Veg oil 25g Carrots 21g Carrots 21g Carrots 21g Carrots 21g Carrots 21g Carrots 21g Oranges Oranges Oranges Oranges Oranges 60g 60g Lentils 60g Beef 60g Beef 60g 55g 95g 55g Beef 55g Spinach Lentils 45g raw 50g Spinach raw 50g Iron (mg) 1. To determine the most appropriate mix, a situation Policies, intervention programs and activities analysis should first be conducted on the magniat the international, national, and community tude, prevalence, and distribution of deficiencies, level are required to effectively alleviate food consumption levels including the intake of micronutrient deficiencies. These efforts include: micronutrients, and food habits and attitudes of vulnerable groups, including socioeconomic data to 1) Increasing the overall quantity of foods conidentify major constraints and opportunities. Benefits of such 6) Food quality and safety issues with implicafood-based strategies include not only improved tions for public health and disease control intakes of specific nutrients but also improved measures to reduce nutrient losses by the overall diets and health status. Strategies to promote dietary diversification National agricultural planning strategies such as within the implementation of food-based apcrop diversification to promote micronutrient rich proaches include: crops, agroforestry, and the promotion of traditional and wild foods can have an impact on the availability of micronutrient foods. Increasing overall food intakes that prohibit urban gardening or which reduce the Micronutrient deficiencies are closely associated availability or sale of fresh foods by street venwith poverty, food insecurity, and undernutrition dors can reduce the availability of micronutrient and are common in those groups whose overall foods. Examining the profitability of producing, food intakes are not sufficient to meet nutritional processing, and marketing such foods and requirements. Seldom is only one nutrient defireviewing the impact of policies on micronutrient cient. Thompson it is likely that multiple deficiencies are also prefoods is key to good health and nutrition. For those with inadequate food intakes, motion of dietary improvement/diversification increasing overall food consumption provides with a focus on improving the intake of bioavailseveral essential micronutrients thereby simultaable iron through greater consumption of animal neously addressing a combination of deficiency products, fruit and vegetables, especially those problems. Promoting consumpgrams need to as a first priority to ensure that tion of micronutrient rich foods fosters better overall food supplies are adequate through overall health for all members of society, provides increasing the production, availability, access to , sustainable improvements by encouraging market and consumption of an adequate and nutritious solutions and long-term behavioral changes diet, especially by those who are hungry and food among high risk groups and is often linked to insecure and most vulnerable to deficiencies. By doing so, food-based strategies address the Efforts to address both increased production root causes of micronutrient malnutrition and assist (supply) and increased consumption (demand) of communities and households to adequately feed food need to be undertaken simultaneously. At the and nourish themselves in both the short and long district and national levels, implementation of large term. Stimulating the small scale agricultural sector scale commercial livestock and vegetable and fruit can produce overall long-term economic benefits production can provide micronutrient foods at reafor those groups dependent upon agriculture for sonable prices. The objective is to provide micronutheir livelihoods and for the economy as a whole, trient rich foods at reasonable prices through effecthereby encouraging sustainable development. Increasing consumption of nantly the urban and non-food-producing rural micronutrient rich foods areas. Commercial oil seed production and red Most traditional diets and food habits provide a palm oil for example can increase the availability of range of nutrients that are able to meet the nutrilow cost dietary fat crucial for the absorption of fat tional requirements of most groups.
Order genuine clozaril online. Five Little Monkeys Jumping on the Bed - Nursery Popular Rhymes - English Song For Kids - Music.