Lisa Giorgina Criscione-Schreiber, MD
- Associate Professor of Medicine

https://medicine.duke.edu/faculty/lisa-giorgina-criscione-schreiber-md
One example is given by O-hydroxybenzoic acid (salicylic acid) in the case of high percutaneous absorption antibiotics in chicken purchase floxin 400mg line, particularly in children treatment for uti medscape buy floxin on line amex. Many of these compounds were originally derived from natural sources antibiotics for acne resistance discount floxin generic, and thus are commonly referred to as fruit acids antibiotic for mrsa safe 400 mg floxin. They are characterized in chemical groups based on the number of carboxylic groups (Table 8 antimicrobial cutting boards floxin 400 mg online. The l-lactic acid produced by the microorganism Lactobacillus is responsible for the taste and odor of sour milk bacteria use restriction enzymes to order floxin without prescription. It is, in addition, an end product of the anaero bic metabolism of the epidermis, present onto the skin surface and in eccrine sweat at low concen tration. The other enantiomer d-lactic acid, also called sarcolactic acid, is formed during anaerobic muscular contraction, and is also found in apples, ergot, digitale, opium, and tomatoes. Mandelic acid (2-hydroxy-2-phenylethanoic acid) is obtained from hydrolysis of bitter almond extracts. Malic acid (2-hydroxy-1,4-butanedioic acid) was frst isolated from unripened apples in 1785. It is widely distributed in plants, particu larly in grapes and the lees of wine. Citric acid (2-hydroxy-1,2,3-propanetricarboxylic acid) was frst isolated from lemon juice in 1784. Biologic Activities of Hydroxyacids A number of biologic aspects of the hydroxyacid action remain unsettled because hasty conclusions were offered from uncontrolled studies. Hence, a wealth of hydroxyacid-enriched cosmetics are present on the market with unsubstantiated claims or little evidence of performance. In some instances, erroneous information and incorrect statements have fourished behind promotional objectives. At least one facet of the hydroxyacid biologic activities is ascribed to the native acid strength of the compounds. This physicochemical characteristic is measured by the proton dissociation in solution, and is expressed by its pKa. The lower the pKa of a hydroxyacid, the stronger its acidic strength: a decrease of 1 pKa unit represents a tenfold increase in the acid strength. If the acid strength infuences some of the biologic effects of hydroxyacids, it does not, however, correlate with the overall potency of the fnal topical formulation. The pH of the formulations varies with both the nature of the hydroxyacid and its concentration. In order to avoid irritation as much as possible, it is desirable to design a cosmetic formulation with a pH close to the physiologic pH range of the skin. Hydroxyacids 85 In order to prevent misunderstandings and misstatements, the biologic activities of hydroxyacids should be evaluated with regard to their chemical structure irrespective of their acidity. The exquisite enantioselectivity exhibited by many biologic systems suggests that enantiopurity is an important parameter in any pharmacological effect including pharmacokinetics, metabolic rate, and toxicity. Thus, the racemic components likely interact differen tially with biomolecules of the skin. Whether such a concern is of importance for the effects elicited by hydroxyacids is not settled. In the feld of benign tumors, keratoses and viral warts are effectively treated by high concentration formulations. The effect of hydroxyacids on actinodermatosis appears more complex, involving multifaceted mechanisms, boosting some of the defcient physiologic aspects of aging skin. In this chapter, the cate gory low concentration is arbitrarily defned when there is less than 4% of active compound in the formu lation. Medium concentration applies to the range 4%?12%, and high concentration for upper dosages. Above this concentration and/or below this pH, they fall under the drug categorization. Their numbers usually decrease towards the surface of the skin, most notably during the stratum compactum to stratum disjunctum transition. One of the main targets is clearly the corneodesmosomes which appear to be weakened following altered chemical bonds in the junctional complexes. In addition, its activity is more closely targeted than that of salicylic acid, because it is channeled into the junction between the corneodesmosome and the corneocyte envelope. The farther away from the physiological pH, the greater the caustic effect, the greater the risk of adverse events, but the more likely the patient receives the resurfac ing benefts of the peeling agents. The indications of such treatment modality encompass the destruction of slightly elevated seborrheic and actinic keratoses. Viral warts are similarly eradicated by hydroxyacids in a home-administered treatment, with applications made daily for several days. To shorten the treatment period, the outer portion of the hyperkeratosis should be removed with a scalpel in an offce setting. Hypopigmenting Effect Glycolic acid peels are a useful adjunctive treatment of epidermal hypermelanosis such as in melasma and acne scars. Acne and Pseudofolliculitis Treatment Salicylic acid is listed among active products to treat acne. Another modality of acne treatment consists of using high concentrations of glycolic acid in an offce setting. In addition to the comedolytic effect, the higher hydroxyacid concentrations help to unroof pustules and affect the follicular epithelium. The skin condition improvement is reported to be precipitous while patients were taking oral tetracyclines. Discomfort, mild diffuse erythema, and fne scaling are often experienced by patients. In addition, there is a risk for stronger irritation leading to a papular and perifollicular erythema that commonly persists for a few weeks. Thus, the compound is likely to be trapped in lesional sebaceous follicles which represent a critical therapeutic target in comedonal acne. The product has shown effcacy in preventing post-summer comedonal acne and in treating mild acne. After a few days of application of 12% glycolic acid at low pH, fne wrinkles of the face may vanish as a result of the irritation and dermal edema. Besides the untoward immediate effect of stinging, such smoothing effect is rapidly alleviated upon arrest of the topical treatment. However, signs of repair and reverse changes of aging and photoaging were reported on long-term therapy. A comparative controlled study showed that tretinoin was more active than medium concentrations of glycolic acid in the improvement of the facial skin tensile properties. Such effects are more evident in older skin and remain within the physiologic range of normal skin. However, the higher concentrations are respon sible for severe redness, swelling (especially in the area of the eyes), burning, blistering, bleeding, rash, itching, and skin discoloration. They concluded that products containing salicylic acid should contain a sunscreen or bear directions advising consumers to use other sun protection. These compounds under the presentation of peels and home regimens are recognized as important preventive means and adjunctive therapy in a variety of skin conditions. Improved regimens capitalizing on the various benefcial effects of hydroxyacids should be explored. Development of a w/o/w emulsion for chemical peeling applications containing glycolic acid. Comparison and correlation between stinging responses to lactic acid and bioengineering parameters. Effects of various concentrations of glycolic acid at the corneoxenometry and collaxenometry bioassays. Clinical tolerance and effcacy of capryloyl salicylic acid peel compared to a glycolic acid peel in subjects with fne lines/wrinkles and hyperpigmented skin. Functional changes in human stratum corneum induced by topical glycolic acid: Comparison with all-trans retinoic acid. Modulation of stratum corneum properties by salicylic acid and all-trans-retinoic acid. Glycolic acid peels versus salicylic-mandelic acid peels in active acne vul garis and post-acne scarring and hyperpigmentation: A comparative study. Effcacy and safety of a new salicylic acid derivative as a complement of vitamin A acid in acne treatment. Increased in vivo collagen synthesis and in vitro cell collagen synthesis and in vitro cell proliferative effect of glycolic acid. Topical 8% glycolic acid and 8% L-lactic acid creams for the treat ment of photodamaged skin. Histometric assessment of the age-related skin response to 2-hydroxy-5-octanoyl benzoic acid. Center for Food Safety and Applied Nutrition Offce of Cosmetics and Colors Fact Sheet. Levy Introduction Retinoids and hydroxy acids have successfully been used as active ingredients to improve the appear ance of aging skin. However, both retinoids and hydroxy acids may be associated with skin irrita tion, stimulating a search for alternatives. Possible alternatives include kinetin (N6-furfuryladenine), zeatin, and pyratine-6. Kinetin and zeatin are members of a plant growth hormone family known as cytokinins, which have growth-promoting and antiaging effects in plants. Pyratine-6 (furfurylamino tetrahydropyranyladenine) is a synthetic analog of kinetin. It is a naturally present base modifcation3 and is present in both plants4,5 and human cell extracts. Zeatin contains adenine with the addition of an hydroxy-methylbutyl group (Figure 9. Cytokinins are plant growth substances that promote cell division and possibly cell differentiation. Plant-based studies are responsible for most of the data regarding the biological properties of kinetin. Low levels of kinetin stimulate calcium infux through plant cell plasma membranes. Both relatively young and old cells were studied: fbro blasts that had completed less than 20% and older cells that had completed 90% or more of their potential in vitro life span were studied (Table 9. The studied cellular manifestations of in vitro aging included cell enlargement, presence of multi-nucleated giant cells, accumulation of cellular debris and lipofuscin, and changes in actin flaments and microtubules. Kinetin did not alter the overall proliferation or the longevity of the cultured cells. Similar results were reported with zeatin with less toxicity at higher concentrations. A diet containing 20?50 ppm kinetin fed to fruit fies prolonged average and maximum life span by 65% and 35%, respectively. Kinetin has inhibitory activity on free radical formation of active platelets in vitro and thrombus for mation in vivo. A cytokinin nucleoside, N6-fufuryladenosine, has been shown to have antiproliferative and apopto genic activity against various human cancer cell lines,17 although similar activity has not been shown with kinetin. Kinetin may function as a natural antoxidant,21 preventing the formation of reactive oxygen species, or as a direct free radical scavenger. However, pluripotency may serve as a required prerequisite to act effectively as an agent of antiaging. There was no signifcant difference in trans dermal absorption with the two test formulations. Topical treatment with low concentrations of kinetin lead to a more homogenous dispersion of melanin granules in the epidermis of dogs as well as reduced the stratum corneum thickness. The overall photodamage was reported 94 Cosmeceuticals and Active Cosmetics improved by both self-assessment and dermatologist grading. Transepidermal water loss was decreased after 24 weeks, which is consistent with an improvement in the stratum corneum barrier function. Ninety-eight subjects with mild to moderate photodamaged facial skin applied a kinetin-containing lotion and creams for 10 weeks (Revlon Research Center, unpublished studies). All subjects were assessed at baseline 4, 8, and 10 weeks for photodamage parameters. Statistically signifcant improvements were noted in all parameters, greatest with texture, skin clarity, discrete and mottled pigmentation, fne wrin kling, and global appearance. Forty female subjects who ranged in age from 22 to 57, having mild to moderate facial skin photo damage, participated in a 12-week, split face, double-blind, controlled, and randomized study compar ing a topical retinol against a topical kinetin-containing lotion twice daily (Almay Research?poster exhibit American Academy of Dermatology meeting, New Orleans, Louisiana, February 2002). Evaluations at four-week intervals demonstrated signifcant improvements for all attributes graded including discrete and mottled pigmentation, fne wrinkling, and overall photodamage. The kinetin containing lotion was found to have greater improvements in texture and clarity. Controlled use testing for up to six weeks demonstrated no signifcant irritation (Almay research, unpublished studies). Subjects were treated with once daily application of 2 mg/cm2 at six sites on the mid back over two weeks. No difference in the minimal erythema dose was demonstrated between untreated control and treated sites. These fndings suggest that kinetin has minimal potential to cause irritation, allergy, or photosensitization. A 12-week open label study on photoaging utilized furfuryl tetrahydropyranyladenine (Pyratine-6).
The lesions appear as small red infection mrsa pictures and symptoms floxin 400 mg online, matologic evaluation in at-risk organ transplant conical antibiotic use in poultry generic floxin 200 mg otc, hard nodules that occasionally ulcerate (Figure 6-33) antibiotics quiz order floxin 400 mg mastercard. Biologic behavior of skin In actinically induced squamous cell cancers antibiotic drops for eyes safe floxin 200 mg, rates of cancer in organ transplant recipients may be aggressive infection 2 bio war simulation buy floxin online now, and metastasis are estimated from retrospective studies to be careful management is required virus 2014 fall cheap floxin 400 mg otc. Interventions for non-metastatic squamous cell carcinoma of the skin: systematic review and pooled analysis of observational studies. Factors predictive of recurrence and death from cutaneous squamous cell carcinoma: a 10-year, single? institution cohort study. Nonmelanoma skin cancer in solid organ trans? plant recipients: update on epidemiology, risk factors, and management. Voriconazole-associated cutaneous malig? nancy: a literature review on photocarcinogenesis in organ transplant recipients. General Considerations Lichen planus is an infammatory pruritic disease of the skin and mucous membranes characterized by distinctive papules with a predilection for the fexor surfaces and trunk. The three cardinal fndings are typical skin lesions, mucosal lesions, and histopathologic features of band? like infltration oflymphocytes in the upper dermis. Lichen? oid drug eruptions can resemble lichen planus clinically and histologically. Hepatitis C infection is found with greater frequency in lichen planus patients than in controls. Allergy to mercury and other metal-containing amalgams can trig? ger oral lesions identical to lichen planus. The lesions are violaceous, fat? topped, angulated papules, up to 1 em in diameter, discrete or in clusters, with very fne white streaks (Wickham striae) on the fexor surfaces ofthe wrists and on the penis, lips, tongue as well as buccal, vulvar, vaginal, esophageal, and anorectal mucous membranes. Mucous membrane lesions have a lacy white network overlying them that may be confused with leuko? plakia. The presence of oral and vulvo-vaginal lichen pla? nus in the same patient is common. Patients with both these mucous membranes involved are at much higher risk for esophageal lichen planus. There is also an increased risk of tion can occur through mucous membranes, serum tacro? squamous cell carcinoma developing in lesions of hyer? limus levels should be checked at least once if widespread trophic lichen on the lower extremities. Differential Diagnosis containing amalgam, removal of the amalgam may result Lichen planus must be distinguished from similar lesions in clearing of the erosions. Lichen planus on the mucous mem? Corticosteroids (see Chapter 26) may be required in severe branes must be differentiated from leukoplakia. Erosive cases or in circumstances where the most rapid response to oral lesions require biopsy and often direct immunofuo? treatment is desired. Unfortunately, relapse almost always rescence for diagnosis since lichen planus may simulate occurs as the corticosteroids are tapered, making systemic other erosive diseases. Hydroxychloroquine, 200 mg orally twice daily, Superpotent topical corticosteroids applied twice daily are acitretin 10-25 mg daily, and cyclosporine 3-5 mg/kg can also most helpful for localized disease in nonfexural areas. Alternatively, high-potency corticosteroid cream or oint? ment may be used nightly under thin pliable plastic flm. Prognosis Topical tacrolimus appears effective in oral and vaginal erosive lichen planus, but long-term therapy is required to Lichen planus is a benign disease, but it may persist for prevent relapse. In the setting of iatrogenic immunosup? tent, and neoplastic degeneration has been described in pression, the treatment of Kaposi sarcoma is primarily chronically eroded lesions. Mucosal lichen planus: an evidence-based treat? accessible and space-occupying lesions; and laser surgery ment update. Cutaneous and mucosal lichen planus: a com? therapy is indicated in patients with rapidly progressive prehensive review of clinical subtypes, risk factors, diagnosis, skin disease (more than lO new lesions per month), with and prognosis. Liposomal doxorubicin is trophic lichen planus: a review and analysis of 38 cases. Paclitaxel and other taxanes can be effective even in patients who do not respond to anthracy? cline treatment. Treatments for classic Kaposi sar? Kaposi sarcoma continues to occur largely in homosexual coma: a systematic review of the literature. Descriptive epidemiology of Kaposi sarcoma in apy, and stopping the immunosuppression may result in Europe. Pulmonary It is modulated by multiple factors, including anxiety, Kaposi sarcoma can present with shortness of breath, depression, and amphetamine and cocaine use. Pruritus as cough, hemoptysis, or chest pain; it may be asymptomatic, a medical complaint is 40% as common as low back pain. Bronchoscopy may be Elderly Asian men are most significantly affected with 20% indicated. Most cases of pruritus are not mediated by ally resembles the endemic form, being indolent and local? histamine, hence the poor response of many pruritic ized. Theses conditions all pres? ent with recognizable cutaneous morphologies, and the treatment of the skin condition usually results in control of the associated pruritus. Examination is highly variable, ranging from no most common cause of pruritus associated with systemic skin findings to excoriations and inflammation of disease is uremia in conjunction with hemodialysis. Naltrexone and nalmefene have been shown to relieve the pruritus of liver disease. General Considerations effective in pruritus associated with advanced chronic Anogenital pruritus may be due to a primary infammatory kidney disease, but gabapentin may be effective. Endo? skin disease (intertrigo, psoriasis, lichen simplex chroni? crine disorders, such as hypothyroidism, hyperthyroid? cus, seborrheic dermatitis, lichen sderosus), contact der? ism, or hyperparathyroidism, psychiatric disturbances, matitis (soaps, colognes, douches, and topical treatments), lymphoma, leukemia, and other internal malignant disor? irritating secretions (diarrhea, leukorrhea, ortrichomoniasis), ders, iron deficiency anemia, and certain neurologic dis? infections (candidiasis, dermatophytosis, erythrasma), or orders may also cause pruritus. Erythrasma (Figure 6-35) is diag? can cause pruritus with or without eczema, even years nosed by coral-red fuorescence with Woodlight and cured after they have been started, and it may take up to 1 year with erythromycin. Squamous cell carcinoma of the anus for the pruritus to resolve after the calcium channel and extramammary Paget disease are rare causes ofgenital blocker has been stopped. Combinations of antihistamines, In pruritus ani, hemorrhoids are often found, and leak? sinequan, gabapentin, mirtazapine, and opioid antago? age of mucus and bacteria from the distal rectum onto the nists can be attempted in refractory cases. In cancer? perianal skin may be important in cases in which no other associated and other forms of pruritus, aprepitant skin abnormality is found. Il-31 blockade may represent a future target of vae does not usually involve the anal area, though anal itch therapy. Up to one-third of causes ofanogenital pruritus may be due to nerve impingements of the lumbosacral spine, Elimination of external factors and irritating agents may so referral for evaluation of lumbosacral spine disease is give complete relief. Pruritus accompanying a specific skin appropriate if no skin disorder is identified and topical disease will subside when the skin disease is controlled. Pruritus accompanying serious internal disease may not respond to any type of therapy. Interleukin-31 is associated with uremic pruritus in patients receiving hemodialysis. Itch as a patient-reported symptom in ambulatory care visits in the United States. Physical findings are usually persistent pruritus ani in patients with atopic dermatitis. Laboratory Findings Microscopic examination or culture of tissue scrapings may reveal yeasts or fngi. Mites, ova, and brown dots of feces (scybala) visi? infection, parasitosis, local irritation from contactants or ble microscopically. Red papules or nodules on the scrotum and on ders of the genital area, such as psoriasis, seborrhea, inter? the penile glans and shaft are pathognomonic. General Considerations Instruct the patient in proper anogenital hygiene after Scabies is caused by infestation with Sarcoptes scabiei. If appropriate, physi? infestation usually spares the head and neck (though these cal therapy and exercises to support the lower spine are areas may be involved in infants, the elderly, and patients recommended. Close physical contact for 15-20 minutes with an infected person is the typical mode of transmission. Facility-associated scabies is increasingly common, primarily in long-term care facilities. Treating constipation, preferably with high-fiber manage? Index patients are usually elderly and immunosuppressed. Instruct the patient to use very When these patients are hospitalized, hospital-based epi? soft or moistened tissue or cotton after bowel movements demics can occur. These epidemics are difficult to eradicate and to clean the perianal area thoroughly with cool water if since many health care workers become infected and spread possible. Women should use similar precautions after uri? the infestation to other patients. Avoid "baby wipes" as they frequently contain pre? servatives that cause allergic contact dermatitis. Symptoms and Signs Pramoxine cream or lotion or hydrocortisone-pramoxine Itching is almost always present and can be severe. Topical doxepin cream 5% is similarly digital spaces of the hands and feet, on the heels of the effective, but it may be sedating. Topical calcineurin inhibi? palms, wrists (Figure 6-36), elbows, umbilicus, around the tors (tacrolimus 0. Underclothing should be changed daily, and in men, the seam of their "boxers" should not rub against or contact the scrotum. Balneol Perianal Cleansing Lotion or Tucks premoistened pads, ointment, or cream may be very usefl for pruritus ani. About one? third of patients with scrotal or anal pruritus will respond to capsaicin cream 0. The use of high? potency topical corticosteroids should be avoided in the genital area. The burrow appears as a short irregular viduals, ivermectin in a dose of 200 meg/kg is effective in mark, 2-3 mm long and the width of a hair. Characteristic about 75% of cases with a single dose and 95% of cases with nodular lesions may occur on the scrotum or penis and two doses 2 weeks apart. In immunosuppressed hosts and those with crusted Hyperkeratotic or crusted scabies presents as thick flak? (hyperkeratotic) scabies, multiple doses of ivermectin ing scale. These areas contain millions of mites, and these (every 2 weeks for two or three doses) plus topical therapy patients are highly infectious. Patients with widespread with permethrin every 3 days to once weekly, depending hyperkeratotic scabies are at risk for superinfection with on degree of involvement, may be effective when topical S aureus, which in some cases progresses to sepsis if left treatment and oral therapy alone fail. Laboratory Findings Oral ivermectin can be very beneficial in mass treat? the diagnosis should be confirmed by microscopic dem? ment to eradicate infections in institutions or villages. Staphylococcal superinfection may lead Best results are obtained when multiple lesions are scraped, to sepsis. In areas where nephritogenic streptococcal choosing the best unexcoriated lesions from interdigital strains are prevalent, infestation with scabies or exposure webs, wrists, elbows, or feet. Patients with hyperkeratotic scabies and associated bacte? rial superinfection may have laboratory findings consistent Gunning K et al. The efficacy oftopical and oral ivermectin inthe Scabies must be distinguished from the various forms of treatment of human scabies. Bedding and clothing should be laundered or cleaned or setaside for 14days inplastic bags. Unless treatment is aimed at all infected persons in a family or institutionalized group, reinfestations will likely occur. Treatment consists of a single on the inner thighs or lower abdomen in pubic application from the neck down for 8-12 hours, repeated louse infestation. Pregnant patients should be treated only if they have documented scabies themselves. General Considerations once for 12 hours-or 5% or 6% sulfur in petrolatum applied nightly for 3 nights from the collarbones down? Pediculosis is a parasitic infestation of the skin ofthescalp, may be used. Body lice usually occur among peo? Patients will continue to itch for several weeks after ple who live in overcrowded dwellings with inadequate treatment. Head lice may be transmitted by shared use of hats or Scabies in nursing home patients, institutionalized or combs. Adults in contact with children with head lice fre? mentally impaired (especially Down syndrome) patients, quently acquire the infestation. There are three different varieties: (1) pediculosis Most failures in normal persons are related to incorrect pubis, caused by Phthirus pubis (pubic louse, "crabs"); use or incomplete treatment of the housing unit. In these (2) pediculosis corporis, causedbyPediculus humanusvar cases, repeat treatment with permethrin once weekly for 2 corporis (body louse); and (3) pediculosis capitis, caused weeks, with reeducation regarding the method and extent byPediculus humanus var capitis (head louse). Trench fever, relapsing fever, and typhus are transmitted by the body louse in countries where those diseases are endemic. Lesions in lineargroups ofthree ("breakfast, lunch, scratching may result in deep excoriations, especially over and dinner") is characteristic of bed bugs. Tender erythematous patches that migrate ("larva Pyoderma may be the presenting sign. General Considerations generalized, particularly in hairy individuals; the lice may Some arthropods (eg, mosquitoes and biting fies) are even be found on the eyelashes and in the scalp. Many others are not because they are too small, because there is no immediate reaction. Reactions are allergic and Head louse infestation must be distinguished from sebor? may be delayed for hours to days. Patients are most apt to rheic dermatitis, body louse infestation from scabies and consult a clinician when the lesions are multiple and pruri? bedbug bites, and pubic louse infestation from anogenital tus is intense. Many persons will react severely only to their earliest contacts with an arthropod, thus presenting pruritic lesions. Sexual contacts should bites; they rarely attack humans, though the brown recluse be treated. Clothes and bedclothes should be washed and spider (Loxosceles laeta, L reclusa) may cause severe dried at high temperature. Malathion lotion 1% (Ovide) der bites (or loxoscelism) are incorrect, especially if made is very effective, but it is highly volatile and fammable, so in areas where these spiders are not endemic.
Purchase floxin with amex. How to Embroider a Towel.
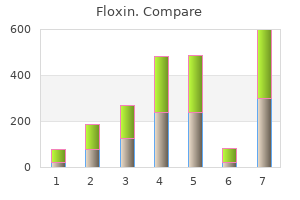
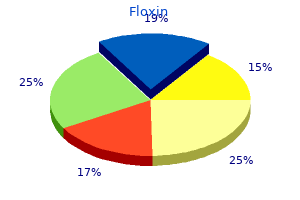
Diabetes prevalence in some Eastern Mediterranean countries is among the highest in the world [3?16] what kind of antibiotics work for sinus infection discount floxin 200mg without prescription. The Eastern Mediterranean Region extends from Pakistan in the east to Morocco in the west zyvox antibiotic resistance generic 200mg floxin visa, and the population is a mosaic of several ethnic groups antibiotics for acne boils proven 400mg floxin. The age distribution pattern of the population is pyramidal antibiotic otic drops cheap 200mg floxin overnight delivery, with about 50% of the population aged below 20 years virus yahoo email floxin 200 mg otc. While the majority of persons with diabetes mellitus in industrialized countries are in the older age group treatment for uti guidelines cheap floxin 400 mg without prescription, the majority in developing countries tend to be middle-aged and at the most productive stage of life [3]. Many Eastern Mediterranean countries are now reporting the onset of type 2 diabetes mellitus at an increasingly young age. Subjects are presenting in their second and third decade, and in some countries type 2 diabetes mellitus is emerging in children. In the Eastern Mediterranean Region as a whole, approximately half of the countries have published incidence rates. The highest rates are reported in Egypt, Kuwait, Lebanon, Oman and Qatar where the incidence of type 1 diabetes is reported to be 8?10 per 100 000 population per year in children aged <15 years while in Pakistan it is only 1 per 100 000 [4?14]. These include progressive urbanization, decreasing infant mortality and increased life expectancy. Increasingly sedentary lifestyles, the obesity pandemic and higher life expectancy have led to a dramatic rise in type 2 diabetes in many countries of the Region [4?14,16]. Traditional activities and dietary patterns that have sustained people over generations are rapidly disappearing and the socioeconomic situation in many countries has forced people to move to urbanized areas to seek employment, where they are less likely to lead a healthy lifestyle. Thus, it is estimated that in the Eastern Mediterranean Region 22 million people (out of a total adult population of 290 million) have diabetes mellitus, and it is predicted that this figure might increase to 30 million by 2025 [2,3]. As in many other countries with high diabetes mellitus prevalence, the onset of type 2 tends to occur at a relatively young age [5,7,10,12]. Regional prevalence of diabetes (%) Country Male Female Afghanistan Bahrain 24. This is particularly true in the areas of screening prevention and early intervention. Diabetes is a costly disease in terms of morbidity, mortality and quality of life. It constitutes a considerable financial burden on individuals, their families, the health sector and governments. In most countries of the Region, specialized diabetes centres are few and far apart and often not within reach of many people with diabetes [2?20]. Likewise, trained and experienced diabetologists are few, nutritionists and diabetes nurse educators are uncommon and chiropodists may be non-existent. Besides, the infrastructure at the primary care level is not capable of allowing meticulous implementation of the routine screening procedures, monitoring control and detecting common diabetes complications. In addition, provision of care for diabetes may differ in the same country, varying from very poor or almost non-existent care in some areas to highly structured care in other places [2]. The majority of Eastern Mediterranean countries were found to have national plans for the prevention of diabetes and had already established national guidelines for the prevention and management (Table 3). More than 50% of Eastern Mediterranean countries reported having diabetes control plans. Effective preventive strategies, therefore, already exist but are not being rationally or widely utilized. The management of diabetes needs to be monitored through implementation of national strategies for optimal control of diabetes, hypertension, dyslipidaemia and obesity. Not only are the risk factors associated with diabetes mellitus ever increasing, but the individual with diabetes frequently makes his or her decisions concerning the disease outside the clinical setting, either at home, on the job, or within his/her existing community. Many individuals are influenced by traditional beliefs, myths and misconceptions regarding the causes, symptoms and care of diabetes mellitus and continue to seek alternative measures for curing their condition. However, the disease is not only a problem for the individual but is also a societal challenge because of its serious complications and cost of treatment. Meanwhile, public awareness and understanding of diabetes remains very low in certain areas. There are many important issues that the Region needs to address, not least of which is the lack of available mortality data. There is also a need for training of health professionals and paramedics on diabetes mellitus prevention and control. There is a lack of information on health care services management for diabetes mellitus as well as a lack of effort to assess the cost-effectiveness of the various interventions [18?20]. The effects of diabetes mellitus include long-term damage, dysfunction and failure of various organs? [21]. Thus, the metabolic abnormalities of diabetes result from inadequate insulin action on target tissues, due to deficient insulin secretion or insensitivity to insulin action, or a combination of both [2,22]. Diagnosis the diagnosis of diabetes in an asymptomatic individual should never be made on the basis of a single abnormal glucose value. Verification of the diagnosis with repeat testing is required, unless an individual presents with unequivocal hyperglycaemia along with its classic symptoms. The diagnostic values for diabetes mellitus and other categories of hyperglycaemia are shown in Table 4. Diagnostic values for diabetes mellitus and other categories of hyperglycaemia [21] Venous plasma glucose concentration mmol/L mg/dL Diabetes mellitus fasting or? Classification the classification of diabetes mellitus has evolved considerably over time, taking into account recent advances in the diabetes field. The classification is now primarily based on the etiology (causes) of the disease, rather than its treatment (Figure 2). The revised classification encompasses both clinical stages and etiological types of hyperglycaemia and results from improved understanding of the causes of diabetes mellitus [21]. The clinical staging reflects that diabetes mellitus, regardless of its etiology, progresses through several clinical stages during its natural history. The severity of glycaemia may change over time depending on the extent of the underlying disease processes. While there are autoimmune markers that help identify type 1 diabetes mellitus, there are few sensitive or highly specific indicators of the type 2 process at present, although these are likely to be revealed in the future. The same disease process leading to type 2 diabetes mellitus can Definition and classification 15 Diabetes mellitus regulation * In rare instances patients in these categories. Disorders of glycaemia: etiological types and clinical stages [21] cause impaired fasting glycaemia and/or impaired glucose tolerance without fulfilling the criteria for the diagnosis of diabetes mellitus. In some individuals with type 2 diabetes, adequate glycaemic control can be achieved with weight reduction, exercise and/or oral agents. Other individuals require insulin for adequate glycaemic control but can survive without it. Terminology There are two main types of diabetes: type 1 (requiring insulin for survival) and type 2 (may or may not require insulin for metabolic control). These terms are confusing and frequently result in patients being classified on the basis of treatment rather than etiology. Type 1 includes those cases attributable to an autoimmune process, as well as those with? Type 2 includes the common major form of diabetes mellitus which results from defect(s) in insulin secretion, almost always with a major contribution from insulin resistance. It has been argued that a lean phenotype 2 diabetes mellitus in adults found in the Indian sub-continent may be very distinct from the more characteristic form of type 2 found in Caucasians. Not enough information is available, however, to characterize such subjects separately [21]. A recent international meeting reviewed the evidence for, and characteristics of, diabetes mellitus in under-nourished individuals. While it appears that malnutrition may influence the expression of several types of diabetes, the evidence that diabetes can be caused by malnutrition or protein deficiency per se is not convincing. Therefore, any decision on screening and Definition and classification 17 intervention has a big implication on resources, as it more than doubles the population eligible for intervention [1,2,23]. A high epidemicity index indicates the beginning of an epidemic and is mostly seen in developing countries. Although this choice is arbitrary, such values have been observed in people with proven normal glucose tolerance; however, others with fasting glucose values <6. Fasting glucose values above this level are associated with a progressively greater risk of developing microvascular and macrovascular complications. In addition, the pathological or etiological process that often leads to diabetes mellitus begins, and may be recognizable, in some subjects who have normal glucose tolerance. Recognition of these processes at any early stage may be useful if progression to more advanced phases can be prevented. Conversely, effective treatment, or occasionally the natural history of some forms of diabetes mellitus, may result in reversal of hyperglycaemia to a state of normoglycaemia [21?23]. An individual with a type 1 process may be metabolically normal before the disease is clinically manifest, but the process of? In some subjects with this clinical form of diabetes, particularly non-Caucasians, no evidence of an autoimmune disorder is demonstrable and these are classified idiopathic type 1. Etiological classification may be possible in some circumstances and not in others. Thus, the category of type 1 diabetes can be identified if appropriate antibody determinations are performed. It is recognized that such measurements may be available only in certain centres at present [23]. Type 2 diabetes mellitus Type 2 is the most common form of diabetes and is characterized by disorders of insulin action and insulin secretion, either of which may be the predominant feature. Both are usually present at the time that this form of diabetes is clinically manifest. The specific reasons for the development of these abnormalities are not yet known [23]. The insulin resistance that occurs in this type is partly explained by the obesity that often coexists with the disease. Other specific types [21?23] Other specific types are currently less common causes of diabetes mellitus, but are conditions in which the underlying defect or disease process can be identified in a relatively specific manner. Chapter 3 Diabetes mellitus in special groups and circumstances Children and adolescents [21] While type 2 diabetes mellitus used to be almost non-existent in children, its prevalence has been increasing rapidly over the past two decades, mostly because of the rapid increase in childhood obesity. A recent study from Taiwan showed type 2 to be the leading cause of diabetes in children aged 6?18 years. In the Eastern Mediterranean Region type 2 diabetes should be screened for in children aged over 10 years if the child is overweight (>120% of the ideal body weight) and if two of the following characteristics are present. Gestational diabetes Background Gestational diabetes is a state of carbohydrate intolerance resulting in hyperglycaemia of variable severity, with onset or first recognition during pregnancy. It does not exclude the possibility that the glucose intolerance may antedate pregnancy but has previously gone unrecognized. The definition applies irrespective of whether or not insulin is used for treatment or whether the condition persists after pregnancy [21,23]. Women who are known to have diabetes mellitus and who subsequently become pregnant do not have gestational diabetes but have diabetes mellitus and pregnancy? and should be treated accordingly before, during and after the pregnancy. Elevated fasting or postprandial plasma glucose levels may well reflect Diabetes mellitus in special groups and circumstances 21 the presence of diabetes that antedates pregnancy, but criteria for designating abnormally high glucose concentration at this time in pregnancy have not yet been established. Nevertheless, normal glucose tolerance in the early part of pregnancy does not itself establish that gestational diabetes will not develop later. It may be appropriate to screen pregnant women belonging to high-risk population groups during the first trimester of pregnancy in order to detect previously undiagnosed diabetes mellitus. Women at high risk who screen negatively and average risk women should be tested between 24 and 28 weeks of gestation [23]. It should be emphasized that such women, regardless of the 6-week post-pregnancy result, are at increased risk of subsequently developing diabetes. This clustering has been labelled diversely as the metabolic syndrome, syndrome X, or the insulin resistance syndrome [21]. Epidemiological studies confirm that this syndrome occurs commonly in a wide variety of ethnic groups including Caucasians, Afro-Americans, Mexican-Americans, Asian Indians, Chinese, Australian Aborigines, Polynesians and Micronesians. In 1988, Dr Gerald Reaven focused attention on this cluster, naming it Syndrome X. Central obesity was not included in the original description, so the term metabolic syndrome is now favoured. Alone, each component of the cluster conveys increased cardiovascular disease risk, but as a combination they become much more powerful. This means that the management of persons with hyperglycaemia and other features of the metabolic syndrome should focus not only on blood glucose control but also include strategies to reduce the impact of other cardiovascular disease risk factors. The metabolic syndrome with normal glucose tolerance identifies the subject as a member of a group at very high risk of future diabetes. Thus, vigorous early management of the syndrome may have a significant impact on the prevention of both diabetes and cardiovascular disease, especially as it is well documented that the features of the metabolic syndrome can be present for up to 10 years before glycaemic disorder is detected. Hypertension Background Macrovascular disease constitutes the major cause of diabetes mortality, with 80% of patients having and/or dying of cardiovascular, cerebrovascular or peripheral arterial disease. Patients with diabetes mellitus exhibit a two to four-fold increase in the risk of coronary events compared to non-diabetic individuals. Although large-scale studies have shown a clear association between improvement in glycaemic control and reduction in microvascular end-organ damage (retinopathy, nephropathy and neuropathy), they have not been able to show a consistent similar relationship between glycaemic control and macrovascular complications. However, many trials have shown a benefit with respect to cardiovascular events, morbidity and mortality when co-existent hypertension is treated. In addition, control of hypertension is also beneficial to microvascular complications.
Lack or additional of a semi-pressure the Non defects in patients of study details trauma patch for 24 hours Patched Group treated with an for (N = 31) antibiotic 93 buy discount floxin on line. The incidence of bacterial keratitis following corneal abrasion is thought to be low antibiotic used for lyme disease buy generic floxin 400mg online, however there may be increased risk with injuries associated with vegetative or organic matter antibiotic resistance research articles buy generic floxin on-line. There also is a reportedly higher incidence of keratitis from foreign body injuries in the developing world than industrialized countries [75][426] east infection buy cheapest floxin. Topical antifungal medications antibiotics for uti make you tired purchase cheap floxin, generally in ointment form antibiotic resistance in the environment buy cheap floxin 200 mg online, have been used to attempt to prevent (or treat) fungal keratitis that typically arises from corneal abrasions with unsanitary objects or sources. Medications (including topical creams) There is no recommendation for or against the use of prophylactic ophthalmic antibiotics for simple corneal abrasion, rust rings, and foreign bodies that do not involve vegetative matter. Strength of Evidence No Recommendation, Insuffcient Evidence (I) Level of Confidence Low? Postoperative Indications: None in the absence of vegetative matter (see below) Benefits: N/A Harms: Potential for allergic reaction Frequency/Dose/Duration: Indications for Discontinuation: Rationale: There are no quality studies suggesting efficacy of prophylactic ophthalmic antibiotics for prevention of eye infections in the setting of minor ocular trauma and not involving vegetative matter; vegetative matter is thought to significantly increase risk of infections and the recommendation is different (see below). There is only one low quality study using antifungals for corneal abrasions which showed lack of efficacy between treatment groups. As there is no quality evidence, antibiotics are not invasive, have few adverse effects and are low cost, there is no recommendation for or against use of antibiotics in the absence of vegetative matter. Of the 38 articles considered for inclusion, 0 randomized trials and 0 systematic studies met the inclusion criteria. Comments: N/A Prophylactic Ophthalmic Antibiotics for Organic Matter Injuries Recommended. Medications (including topical creams) Prophylactic ophthalmic antibiotics are recommended for abrasions associated with significant organic or vegetative matter. Postoperative Indications: Abrasions due to organic or vegetative matter, regardless of whether a foreign body removal procedure was required. However, there is thought to be considerably higher risk of infection when vegetative matter is involved due to potential microbial load/dose, and this is thought to increase risk of infection. Ophthalmic antibiotics are noninvasive with low risk for systemic effects, but do carry small risk of adverse events such as allergic reaction, eyelid itching and swelling, and conjunctivitis. Costs range from inexpensive to relatively high cost for new wide spectrum antibiotics. Eye injuries associated with plant or vegetative matter or organic matter likely have higher risk for bacterial or fungal infection and may warrant use Copyright 2017 Reed Group, Ltd. Postoperative Indications: Rust ring with or without foreign body removal with larger sized ocular trauma. Ophthalmic drops were evaluated in one moderate quality study after rust ring removal and found evidence of efficacy [411]. Of the 38 articles considered for inclusion, 8 randomized trials and 0 systematic studies met the inclusion criteria. Brown Clinical No mention N = 121 with Slim electric drill Follow-up daily until Manual breakup The dental burr Unclear if 1975 trial of significant corneal treatment group eyes had healed. Rust (score = sponsorship rust rings and removing foreign firm stromal drill is the quickest, removal via drill 6. Manual with manual treatment for manual treatment group treatment corneal rust rings. It removal, though removing foreign compared with enables complete not statistically body with 40 mm x electric, causing removal of the significant. No Follow up conducted further significant by phone interview differences were rather than found. Therapy, removal of rust and the Sam slit-lap (4000 cps) ring from however, is effective rings with S. Shubert examination, treatment group treatment within only as long as re Deferoxamine Foundation, visual acuity and (10% deferoxamine 8 days; 4 between epithelialization is dependent on Inc. No p-value the drug through an rings require statistics intact epithelial more days for reported. Medications (including topical creams) the use of topical antifungal medications is not recommended for routine prophylaxis of simple corneal abrasions, rust rings and foreign bodies. They may be of benefit in select populations at risk for contaminated injuries such as from plants or organic matter. Strength of Evidence Not Recommended, Insuffcient Evidence (I) Level of Confidence Low? Postoperative Indications: Not indicated for simple abrasions, rust rings and foreign bodies. Benefits: N/A Harms: N/A Frequency/Dose/Duration: N/A Indications for Discontinuation N/A Rationale: There are no quality trials of efficacy in a developed country. There is one moderate quality comparative trial comparing use of antibiotics and topical clotrimazole with antibiotics in a developing world tribal population [427]. The study may be limited by power, generalizability from Southern India, potentially different foreign body source(s) and/or complications may have differed [427]. Topical prophylactic antifungal medications are noninvasive, have low risk for adverse events, low to moderate cost, and are not shown to be effective and thus are not recommended for routine use as prophylaxis for simple corneal abrasions. Study Care System, with fluorescein received between village setting using may not be and Lions stain and a blue chloramphenicol groups. Therapeutic Contact Lens for Corneal Abrasions, Rust Rings, and Foreign Bodies Not Recommended. Devices A therapeutic contact lens or contact bandage is not recommended for corneal abrasions, rust rings, or foreign bodies. Strength of Evidence: Abrasions Not Recommended, Evidence (C) Strength of Evidence: Rust Rings, Foreign Bodies Not Recommended, Insuffcient Evidence (I) Level of Confidence Moderate? Postoperative Indications: Generally not indicated for corneal abrasions, rust rings or foreign bodies as a stand-alone treatment Benefits: None Harms: N/A Frequency/Dose/Duration: N/A Indications for Discontinuation: N/A Rationale: There is one moderate quality trial that compares use of patching with therapeutic contact lens and topical antibiotic for healing rates of simple corneal abrasion. The encoded proteins act as a mitogenic factor that responds by initiating cellular growth. Strength of Evidence: Abrasions Not Recommended, Evidence (C) Strength of Evidence: Rust Rings, foreign bodies Not Recommended, Insuffcient Evidence (I) Level of Confidence Low? Postoperative Indications: Not indicated for the treatment of corneal abrasions, rust rings and foreign bodies. Of the 38 articles considered for inclusion, 1 randomized trial and 1 systematic study met the inclusion criteria. Placebo, disorders requiring containing only substantial cell the drug vehicle proliferation. These medications are typically applied directly to the eye to assist with eye examinations or surgeries, and to treat cyclitis and iritis. Mydriatic Medications for Simple Corneal Abrasions, Rust Rings, and Foreign Bodies Moderately Not Recommended. Medications (including topical creams) Mydriatic medications are not recommended for treatment of simple corneal abrasions, rust rings and foreign bodies. Strength of Evidence Moderately Not Recommended, Evidence (B) Level of Confidence Moderate? Postoperative Indications: N/A Benefits: N/A Harms: N/A Frequency/Dose/Duration: N/A Indications for Discontinuation: N/A Rationale: There is one high quality trial demonstrating no efficacy of mydriatic medication compared with synthetic teardrops for analgesia after corneal abrasion. The use of mydriatic medications for corneal abrasion is not recommended except in circumstances that require pupil dilation. There are 8 moderate and low quality trials that utilized mydriatic medications in conjunction with other treatments with no comparison of efficacy. These articles are found in other tables elsewhere in this guideline or the appendix. Of the 38 articles considered for inclusion, 1 randomized trial and 8 systematic study met the inclusion criteria. Artificial tears or lubricants are often used to relieve eyes exhibiting dryness, or keratoconjunctivitis sicca, when the eyes are unable to produce adequate tears. Artificial Tears or Lubrication for Extensive Corneal Abrasions, Rust Rings, and Foreign Bodies Recommended. Strength of Evidence Recommended, Insufficient Evidence (I) Level of Confidence Low? Postoperative Indications: Corneal abrasions of sufficient size and pain that require adjunctive treatment. There is insufficient evidence for or against use of artificial tears, and other interventions may be more beneficial. Of the 38 articles considered for inclusion, 2 randomized trials and 2 systematic studies met the inclusion criteria. The They may act as a corneal tears 4 times per number of substitute for oral abrasions. Pain can be induced from the presence of foreign bodies, corneal abrasions and many other conditions [440]. Use of Topical Anesthetics for Corneal Abrasions, Rust Rings, and Foreign Bodies Moderately Recommended. Medications (including topical creams) the selective use of topical anesthetics as a patient treatment option is recommended for short-term analgesia for corneal abrasion, rust rings and foreign bodies. The prolonged use of topical anesthetics is controversial, with concerns for toxicity from overuse, or complications from overtreatment of pain such as retained foreign body. Topical anesthetic is not invasive, has low but potentially important adverse effects and is generally low cost. Of the 38 articles considered for inclusion, 3 randomized trials and 2 systematic studies met the inclusion criteria. Mean proparacaine (N days 1, 3 and 5 5 minutes after anesthetic is an limits conclusion. Color after administration efficacious analgesic Numbers enrolled for proparacaine and smell enrollment. Larger acetaminophen studies powered for with 30 mg of safety are necessary codeine for before widespread breakthrough adoption of this pain; topical practice. Extended chronic use can result in adverse effects to the corneal tissues reportedly including alteration of lacrimation, corneal sensitivity loss, increased corneal permeability, disruption of corneal cell motility, swelling and corneal re-epithelialization inhibition [442]. Topical Opioids for Analgesia of Corneal Abrasions, Rust Rings, and Foreign Bodies Not Recommended. Medications (including topical creams) the use of topical fentanyl and opioids for analgesia of corneal abrasions, rust rings, and foreign bodies is not recommended. Strength of Evidence Not Recommended, Evidence (C) Level of Confidence Moderate? Postoperative Indications: N/A Benefits: N/A Harms: Decreased lacrimation, corneal sensitivity loss, increased corneal permeability, disruption of corneal cell motility, swelling and inhibition of corneal re-epithelialization. Frequency/Dose/Duration: N/A Indications for Discontinuation: N/A Rationale: There is one quality trial comparing the use of topical fentanyl with no fentanyl that demonstrated no improved in analgesia at the dose tested. These medications are not invasive, have reported adverse effects, and have no demonstrated efficacy and are thus not recommended. Of the 38 articles considered for inclusion, 26 randomized trials and 8 systematic studies met the inclusion criteria. Group B: groups: Group fibers within the suggest no Forschungsgemeinschaft mean age 0. Patients with minor abrasions may require no follow-up other than if symptoms persist and fail to resolve in one to two days. Patients with more extensive abrasions, abrasions from vegetative matter, large foreign body removals and/or large rust ring removals may require followups every 1-3 days until healed. The primary purposes of frequent followup appointments are to assess healing, detect complications and address work limitations all of which may change quickly. These are diverse and complex injuries that include a range of injuries from simple corneal lacerations to deep structural injuries. Complications of these injuries include visual impairments, astigmatisms, endophthalmitis, infections, sympathetic ophthalmia, cataracts, blindness, and enucleation [371, 447, 448]. Corneal Lacerations Corneal lacerations are deeper wounds than abrasions and include flap wounds. More extensive wounds may include injury to intraocular structures such as the lens. Retinoic acid has been used for adjunctive treatment of corneal lacerations [449], however, there are no quality studies and it is Recommended, Insufficient Evidence (I). Rigid gas-permeable contact lenses have been used to attempt to provide better healing [450-453]. There are no quality studies of contact lenses for this purpose, and they are Recommended, Insufficient Evidence (I). Penetrating trauma and intraocular foreign bodies are Recommended, Insufficient Evidence (I) to be initially treated with stabilization of the intraocular foreign body without removal to avoid further trauma, and prompt, emergent referral for definitive treatment. Many small intraocular foreign bodies, particularly metallic, do not require removal, and instead can be conservatively managed [454-456]. This guideline does not address these penetrating eye injuries in detail that require referral for highly individualized, definitive care [367, 455, 457-470]. Blunt Trauma and Traumatic Hyphema Blunt ocular trauma is most commonly due to transportation crashes, sports injuries and altercations [84, 471, 472]. Other occupational causes occur beyond those due to work-related vehicular crashes [84, 473]. Predictors of worse outcomes reportedly include afferent or nonreactive pupil, fracture, and inability to open the eye [474]. Blunt trauma injures are highly diverse and include contusions, fractures, hyphema, retinal detachments, anterior chamber angle recession, ocular hypertension, and other complications [72, 475, 476]. As multiple other injuries are potentially present, a comprehensive evaluation of the patient and his/her neighboring tissues/organ systems is required. Orbital blowout fractures most commonly involve the medial wall followed by the orbital floor [473]. Prevention of re-bleeding is believed to be important to prevent worse outcomes and prednisone and aminocaproic acid have been utilized.